Introduction
Informal caregivers (e.g., spouses and children of care recipients) provide critical and ongoing social, emotional, and instrumental support to their adult family members with chronic health conditions.1,2 Although caregiving can be rewarding,3,4 studies have found that caring for an adult with chronic conditions is associated with increased psychological distress, lower quality of life, and diminished participation in meaningful and personally valued activities.5–9
Family caregivers often encounter challenges in their caregiving situations.10 They tend to delay or place a low priority on taking care of themselves,11,12 which can worsen their health and well-being.13 These effects on caregivers can ultimately have a negative impact on care recipients. Studies have shown that psychological distress among family caregivers related to caregiving was associated with poorer outcomes for the care recipient, including increased depressive symptoms, anxiety, and behavioral problems and poorer functioning and quality of life.14,15 Therefore, it is essential to understand how these caregiving experiences affect the physical and mental health and well-being of these caregivers to develop and strengthen interventions that support them.
The daily experiences of family caregivers, including those of adults with chronic health conditions, often fluctuate in response to changes in care demands, situations, and activities.16 Ecological momentary assessment (EMA) captures these day-to-day changes at different moments17,18 and therefore has the potential to enhance the sensitivity of data collected from caregivers. EMA, or experience sampling method (ESM), is a data collection method that involves frequent and repeated assessment of momentary experiences in an individual’s natural environment over a defined time.19,20 EMA collects a representative sampling of the respondents’ experiences under different circumstances to measure fluctuations in behaviors, emotions, and thoughts over time.21
Researchers using EMA generally send brief surveys to participants’ mobile devices (e.g., smartphone) at several random or predetermined times a day to check their in-the-moment experiences in certain situations (e.g., a specific location or social companion).21–24 Typically, EMA notifications prompt participants to respond immediately (i.e., within minutes) to survey questions.25 Participants can access and complete surveys through a preprogrammed application or a web link to an online platform.
EMA has a number of advantages. It assesses behaviors, emotions, and thoughts in the moment and in the social and environmental context in which the behaviors occur. This produces ecologically valid data that are less influenced by retrospective recall bias compared to traditional daily self-report measures, which are generally completed at the end of the day or even after several days. EMA also facilitates the exploration of temporal relationships among variables (e.g., psychological states and situations), reveals frequency and patterns of daily fluctuations in individuals’ experiences under different circumstances over time, and measures the effects of psychosocial interventions.26–28 The benefits of EMA also include its potential to increase the accuracy of participant-reported outcomes compared to traditional methods of identifying changes in response to an intervention.16,29–32 With EMA, respondents cannot access or alter their previous answers, and data have shown that in-the-moment reports of activities and behaviors are more accurate than retrospective reports.33 Likewise, studies have shown that EMA-based evaluations of the effects of psychosocial interventions were more sensitive to change than retrospective self-report questionnaires or one-time daily diaries.27
Previous systematic reviews have identified and summarized studies that used EMA as a data collection method for outcomes of interventions for specific populations, such as people with major depressive disorders34 and middle-aged and older adults.35 Findings from these previous systematic reviews support the feasibility and acceptability of using EMA as a data collection method in several populations. To our knowledge, no systematic reviews have been conducted to summarize studies using EMA completed by family caregivers of adults with chronic health conditions.36,37 This systematic review, therefore, aims to synthesize studies that involved EMA completed by family caregivers of adults with chronic health conditions.
Methods
This systematic review was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline.38
Search Strategy
We identified relevant articles by searching six electronic databases (Academic Search Premier, CINAHL, EMBASE, PsycINFO, PubMed, and SCOPUS) from the date of inception of each database through September 15, 2023. To identify potentially relevant publications involving EMA, we constructed our queries for title and abstract screening using Boolean combinations of the following key search terms: (“ecologic* momentary assessment” OR “electronic momentary assessment” OR “momentary data” OR “experience sampling” OR EMA OR ESM OR “ambulatory assessment*”) AND (“caregiv*” OR “carer*” OR “informal care*” OR “family care*”). To identify additional potentially appropriate studies, we manually searched reference lists of selected articles, relevant scoping or systematic reviews, and related review articles identified in the databases.
Eligibility Criteria
We used the following inclusion criteria to select studies: (a) EMA methods completed by family caregivers of adults with chronic conditions; (b) report of EMA outcomes of caregivers’ self-reported activities, behaviors, emotions, or well-being; and (c) written in English and published in a peer-reviewed journal with full text available. Studies were excluded if they (a) were case reports, studies with a sample size less than ten, study protocols, qualitative studies only, dissertations, conference abstracts, book chapters, commentaries, conceptual papers, review articles, or secondary analyses of an original study using EMA methodology (i.e., duplicates in terms of population, methodology, and EMA outcomes); (b) collected data through end-of-day daily diaries, which involves surveying participants once a day for several days39; (c) included only proxy-reported EMA outcomes of care recipients or reports of care recipients’ behaviors from caregivers’ perspectives; or (d) involved care recipients who were not adults or were related to parenting children with chronic health conditions.
Data Extraction and Quality Assessment
We extracted characteristics of the included studies into a table, including publication information, study design, and purpose of the study, demographics of participants (i.e., family caregivers), description of interventions (if applicable), EMA methods and measures, compliance rate, and relevant findings. We used items from the Checklist for Reporting EMA Studies (CREMAS) to determine the quality of the included EMA studies. CREMAS was developed to enhance the reliability, efficacy, and interpretation of findings from studies involving EMA.40 The CREMAS items for this review included device/technology used, number of rating questions/items asked, frequency of daily prompts, duration (i.e., number of days) of prompt monitoring, total number of prompts, prompt design (i.e., fixed or random intervals), and rate of compliance with EMA prompts.40
Study Selection Process
We conducted a two-phase screening process of the retrieved articles. In the first phase, we reviewed titles and abstracts of all retrieved articles to determine whether they fulfilled eligibility requirements. In the second phase, we downloaded and reviewed the full text to verify information in abstracts that suggested the article met eligibility criteria. Two authors (AH and HKY) conducted both phases independently to minimize the exclusion of any relevant articles that met eligibility criteria. We used EndNote 20 (bibliographic software) to manage retrieved articles and eliminate duplicates. After identifying the final number of eligible articles for assessment, two authors (LAM and HKY) used CREMAS to evaluate the quality of each article. The authors discussed all disagreements related to the selection of studies or appraisal of quality until they reached a consensus.
Results
Selection of Studies
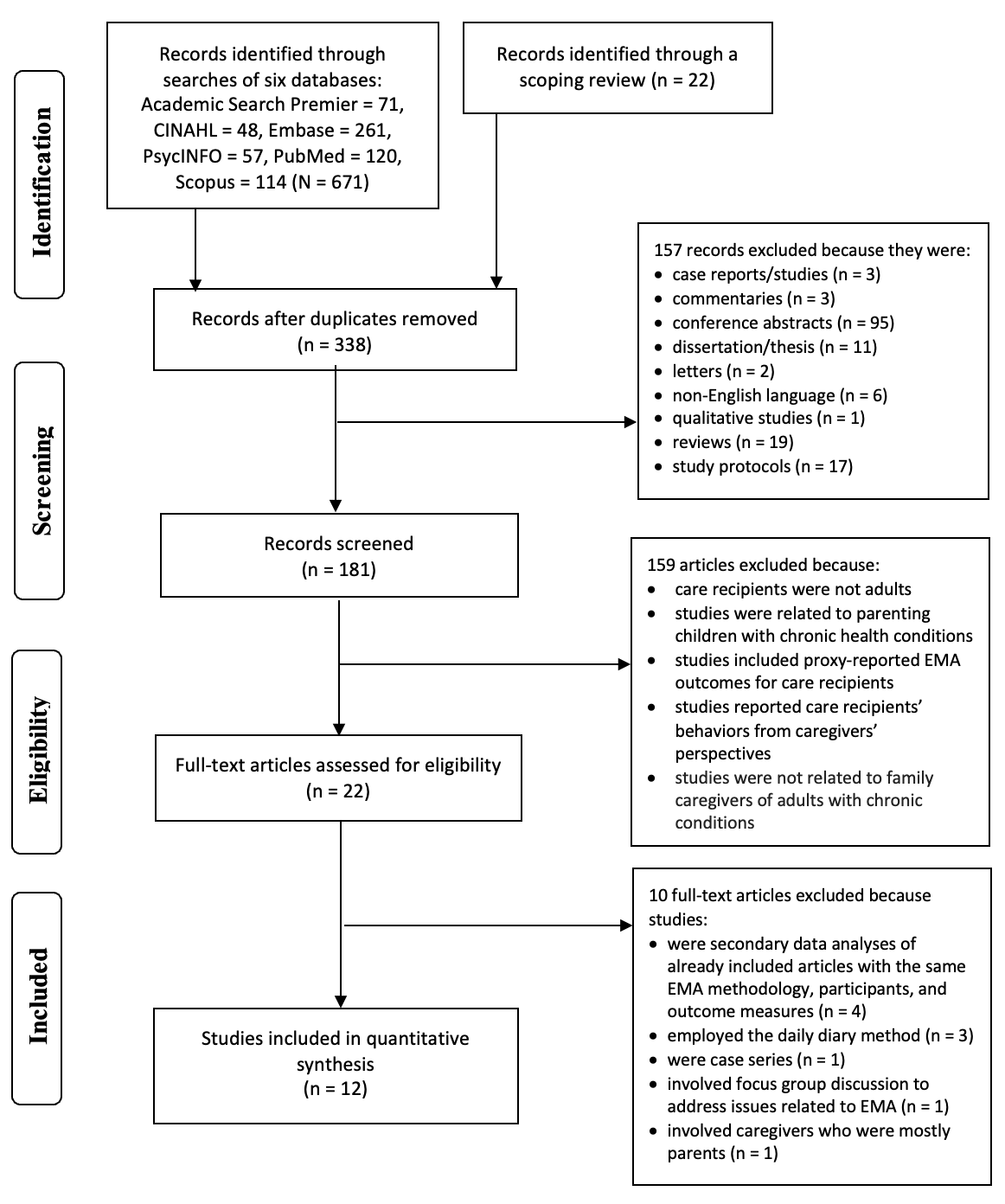
The flow diagram in Figure 1 describes the study selection process and the results of the literature search and data extraction. A total of 671 articles were identified through database searching, and an additional 22 were identified using the reference list from a scoping review.37 After removing 355 duplicates, we disqualified another 157 articles due to the research design, types of publication, or because they were not appropriate for systematic review. We screened 181 articles identified through title and abstract screening and excluded 159 of these because they did not meet eligibility criteria. We read the full text of 22 articles to assess their eligibility for inclusion and excluded ten of these for the following reasons: four16,41–43 were secondary data analyses of articles already included in the current review and had the same EMA methodology, participants and outcome measures; three29,44,45 used the daily diary method; one was a case series with a sample size less than ten46; one involved focus group discussion to address issues related to EMA,18 and one included caregivers who were mainly parents and grandparents.47 A total of 12 studies met the eligibility criteria for the present review.

Characteristics of the Included Studies
The main characteristics of the 12 included studies are summarized in Table 1. Of the 12 included articles, six17,25,48–51 were descriptive studies, two52,53 were comparative (observational) studies, two used a pretest–posttest design,54,55 and two56,57 were randomized controlled trials (RCTs). Only one57 examined the efficacy (sense of competence and mastery, perceived stress, depression, and anxiety) of an EMA-based intervention (EMA self-monitoring and personalized feedback sessions with a coach). The total number of caregiver participants included was 461, with a range from 15 to 76 participants. The mean age of the caregivers was 65.3 years. The proportion of female caregivers included in the studies ranged from 61.3% to 96%, with a mean of 78.1%. The ratio of spousal caregivers to child caregivers was 3.8:1.
Ten studies involved EMA completed by family caregivers of people with Alzheimer’s disease or dementia,17,25,29,44,48,52,54–57 one involved EMA completed by family caregivers of people with cancer50; and one involved caregivers of people with Alzheimer’s and other chronic illnesses.49 Seven studies included caregivers who were either the spouse or child of the care recipient,17,50–52,54–56 four studies25,49,53,57 involved spousal caregivers only, and one study did not report the family relationships of caregivers to care recipients.48
Using CREMAS, studies were evaluated considering their characteristics and EMA methods (i.e., device/technology used; prompt design; frequency of daily prompts; duration of prompt monitoring; and compliance rate). To give prompts for EMA data collection, studies used smartphones (automatic signaling, n = 2),50,56 personal digital assistants (PDAs, n = 4),25,49,52,57 tablet/iPad (n = 1),17 email (n = 1),51 and phone calls (n = 1).53 Three studies did not mention the use of any device to prompt caregiver participants to complete surveys.48,54,55 Five of the 12 studies gave caregivers prompts at time-contingent or prescheduled times48,50,51,53,56 and five used random or semi-random prompts.17,25,49,52,57 Three studies instructed participants to complete questions via pencil-and-paper at fixed times each day.48,54,55 Four studies48,51,54,55 featured retrospective responses and one17 was considered event contingent. The caregivers received an average of six prompts per day, with a range from two to ten daily prompts. Study durations varied from 1 day to 12 weeks, with a mean duration of 15 days. The average number of EMA prompts was 76.6 with a range from 3 or 4 to 304 prompts. Given that one study54 did not report the rate of compliance with EMA prompts, the average compliance rate with EMA prompts for the eleven studies was 75% (standard deviation = 11%), with individual study rates ranging from 59% to 92.7%. The average number of questions requested for the caregiver participants to answer through EMA was 16.5, ranging from 1 to 43 in each assessment. The outcomes reported by family caregivers in EMA included: affect or mood,25,48–50,53,56,57 stress,25,51,52,54–56 well-being,53,57 care demand,52 and fatigue.52
Discussion
This systematic review identified 12 studies that used EMA methods completed by family caregivers of adults with Alzheimer’s or dementia (ten), with cancer only (one), and with multiple health conditions (one) and reported study-specific outcomes (e.g., affect, stress, well-being, care demand, and fatigue). The 12 included studies focused mainly on family caregivers of adults with Alzheimer’s disease and dementia highlighting a gap in the literature, which indicates a need for EMA studies of family caregiver populations in which care recipients have other specific chronic conditions, such as amyotrophic lateral sclerosis, severe intellectual disability, and serious mental illness. Such investigations are needed as the experiences of family caregivers may differ in response to the unique daily demands and activities involved in caring for a person with a specific chronic condition (i.e., condition-specific needs).
A majority of the included studies adhered to the EMA method items from CREMAS. Studies involving EMA conducted before smartphones were widely available often provided prompts and collected data using PDAs or tablets/iPads. All EMA studies published after 2020 used smartphone-based EMA, which is thought to capture the patterns and fluctuations of each caregiver’s experience more accurately. However, most of the included studies did not collect the daily activities and care contexts of the family caregivers in their responses to the EMA prompts.
The nature of the relationship between caregivers and care recipients (e.g., a care recipient’s spouse versus their child), the age of caregivers, and the involvement of other family members in the home are crucial factors that can affect caregiver burden and emotions. In addition, the time-of-day data are collected (morning versus evening, when care recipients may exhibit sundown syndrome behaviors) is likely to produce variable responses. Therefore, it is important for future studies involving EMA to compare and evaluate the burden or emotions of varied groups of caregivers at different times of day, as well as to investigate interactions between caregivers and care recipients over time and to predict and monitor treatment response.
The number of surveys per day, as well as the number of days that data were collected, varied among the included studies. One study collected data for 1 day only, and participants were asked to complete the questionnaire three to four times in one day,52 a design that does not align with the longitudinal nature of EMA. Caregivers often serve their family members in long-term situations, however, none of the included studies tracked the caregivers’ experience using EMA for more than 12 weeks. Therefore, these studies may provide limited insight into the changing experiences and their impact on the emotional experiences and well-being of the caregivers across an extended period.
One study collected EMA assessment data only when the participants were using the app on an iPad.17 As a result, the participants’ responses reflected only their activities while they were using the iPad, which may not represent their responses when doing other activities or at different times of the day. Remote health data collection technology can help overcome this limitation by facilitating investigation of EMA measures using electronically activated recorder-observed behavioral data58 such as heart rate and blood pressure collected using smartwatches worn by caregivers. For example, a study using this technology prompted caregivers to complete a short survey (i.e., deliver EMAs) about their current situation and its antecedents, such as care recipients’ behaviors, when smartwatches detected that the caregiver had an abnormally high heart rate.59 Examining the self-reported intensity and variability of caregivers’ positive and negative emotions across caregiving contexts using EMA will help clinicians better understand coping among caregivers, which has important implications for developing interventions that can improve the quality of the relationships between caregivers and care recipients.
Three studies used a paper and pencil format to collect data for 4 to14 days.48,54,55 These studies did not provide daily sound notifications of prompts but requested that participants complete a paper and pencil questionnaire every 2 to 3 hours during the day.48,54,55 These methods for the submission and collection of data introduced the possibility that participants forgot to complete questionnaires, retrospectively completed them based on recall, or adjusted their previous responses before submission. The authors of these studies acknowledged the limitations of these traditional assessment approaches.
Nine (75%) of the included studies provided no more than six signal prompts per day, which is the suggested maximum considered appropriate to avoid overburdening participants.60 Although no gold standard exists, compliance rates (rates of participant compliance with EMA prompts) of at least 80% have been recommended.61 Previous systematic reviews of EMA studies in other populations have found that the average compliance rate with EMA prompts across studies was lower than the recommended rate, ranging from 71% to 78.4%.40,61 In this review, the mean and standard deviation compliance rate across the included studies was 75±11%, ranging from 59% to 92.7%. Since compliance with EMA protocols may be affected not only by prompting designs (e.g., frequency and duration) but also by participant characteristics,61,62 further studies are needed to consider these factors in the design of EMA protocols. Based on the response rate identified in this systematic review, the use of EMA in research involving caregivers of adults with chronic conditions is feasible and acceptable. However, repeated measurement may lead to changes in participants’ responses (i.e., practice effect), and none of the included studies addressed this possibility.
This review also found few experimental studies involving EMA-based interventions for family caregivers of adults with chronic conditions. Of the 12 studies included in the current review, only one57 involved EMA-based interventions. Findings from this study indicated that EMA-based interventions may help family caregivers improve the management of their daily lives and their health and well-being.57 Further studies are needed to develop tailored protocols for EMA-based interventions to meet the different needs of family caregivers and to examine the efficacy of EMA-based interventions in this population.
Overall, this systematic review showed the use of EMA to collect information of family caregivers of adults with chronic health conditions appeared feasible and acceptable. However, the methodology or design of using EMA to collect caregiver information in this population is still in the preliminary stage. The limited number of existing studies that have used EMA to capture the daily experiences (i.e., activities and care contexts) of family caregivers does not provide key information that could improve understanding of caregivers’ real-life situations. Some of the most influential events may be uncommon or brief (e.g., conflicts and happiness), and the reviewed studies may have failed to capture them. In addition, they did not assess how coping differs among groups of caregivers and with varied mixes of gender family relationships between caregivers and care recipients. More studies employing EMA as outcomes or interventions are needed to improve understanding of the evidence and inform research and practice to support the health and well-being of family caregivers of adults with chronic health conditions.
Limitations: The present systematic review has some limitations. It includes only studies indexed in the selected electronic databases. In addition, the included descriptive, comparative, and experimental studies were heterogeneous, and only one involved an EMA-based intervention, which ruled out a quantitative meta-analysis focusing on the associations among specific variables or the effects of EMA-based interventions. Therefore, the results are presented in narrative form.
Disclosures about potential conflict of interests
None
Authors’ contributions
-
Substantial contributions to the conception or design of the work: AH, HKY, HYL
-
Substantial contributions to the acquisition: AH, LAM, HKY,
-
Substantial contributions to the analysis or interpretation of data for the work: AH, LAM, HKY, JG, RH, XZ
-
Drafting the work or revising it critically for important intellectual content: AH, LAM, HKY, JG, RH, XZ
-
Final approval of the version to be published: AH, LAM, HKY, HYL, JG, RH, XZ