1. Introduction
Domestic violence is a widespread and complex social problem that affects individuals, families, and communities worldwide. According to the World Health Organization (WHO), it is understood as a behaviour focused on the oppression of a member of his family, causing significant harm and trauma through physical, sexual, and mental damage.1
Statistics show that domestic violence is widespread in all ages, ethnic groups, and economic classes.2 In terms of gender, about one in three women worldwide has experienced physical or sexual violence from an intimate partner, with even higher rates reported in some countries3; however, men can also be victims of domestic violence, with estimated prevalence rates ranging from 10 to 50 percent.4 Lately, research is focusing on domestic violence with male victims, an apparently growing phenomenon.5
Experiencing domestic violence can have severe and long-lasting consequences for victims’ physical and mental health, including increased risk of injury, depression, anxiety, post-traumatic stress disorder (PTSD), and other psychological problems.6–8 Compared to the consequences on physical health, mental illness may be less visible or tangible to the victims themselves and to society. Research has shown that 75% of people seeking help from domestic violence support services have clinical symptoms of post-traumatic stress, with depression and even more severe anxiety cases.9
Peritraumatic distress is defined as the emotional and physiological distress experienced during, and/or immediately after, a traumatic event and it is associated with the development and the severity of post-traumatic stress disorder and other mental health problems, among victims of domestic violence.10,11 The intensity of peritraumatic distress is significantly linked to the intensity of PTSD symptoms.12 Studies of peritraumatic responses have shown that a variety of physiological, emotional, and cognitive responses occur in the context of exposure to a trauma. These include increased emotional and physiological excitement, such as a sense of personal life threat, fear; feelings of impotence, horror, guilt, and anger.13
The research on peritraumatic distress among victims of domestic violence has primarily focused on women, with limited attention given to men’s experiences. Gender differences in peritraumatic distress may have important implications for interventions and treatment outcomes, as men and women may respond differently to trauma and may have distinct needs and challenges.14
About the gold standard therapies, out of the many treatments researched, the trauma-focused therapies showed the most benefit in treatment. More research needs to be conducted to directly discover and address the reasons underlying the lack of broader availability of manualized trauma focused therapy by therapists. For those desiring such, or in the absence of good access to trauma focused therapy there is also strong evidence for use of Selective Serotonin Reuptake Inhibitors (SSRIs) and Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs) such as fluoxetine, paroxetine, sertraline, and venlafaxine, and at appropriate doses will assist with symptom reduction. SSRIs and SNRIs are types of antidepressant medications commonly used in the treatment of trauma-related disorders, such as PTSD.15 Both types of medication can help alleviate symptoms of depression, anxiety, and PTSD by regulating the levels of these neurotransmitters in the brain. They can help reduce the intensity and frequency of intrusive thoughts, flashbacks, and nightmares, as well as improve mood and decrease feelings of anxiety and agitation.16,17
Therefore, the current study aims to examine gender differences in peritraumatic distress among men and women victims of domestic violence. Specifically, we will explore the cognitive, emotional, and physical domains of peritraumatic distress and their relationship with the severity of domestic violence and social support. We will also investigate the most frequent type of aggressor in the sample. Findings from this study may inform the development of gender-sensitive interventions that effectively address the unique needs and challenges of men and women who have experienced domestic violence.
2. Materials and Methods
In 2019, we conducted an investigation in the Emergency Medicine Department of Catania Territory, Sicily (Italy), where patients experiencing shock due to domestic violence were treated by first aid doctors for physical injuries before being referred to a qualified psychologist for further assistance. Psychologists and psychotherapists at the emergency department provided psychological support counselling to calm patients and administered a psychological test to evaluate possible post-traumatic distress. The Peritraumatic Distress Inventory (PDI)18 was used to assess the level of distress experienced by the patient during or immediately after the potentially traumatic event. The PDI is a self-report instrument consisting of 13 items scored on a 4-point Likert-type scale, ranging from 0 to 4 (0 = not at all, 1 = slightly, 2 = somewhat, 3 = very, and 4 = extremely true), with the total score ranging from 0 to 52 and higher scores indicating greater distress.
Items explore cognitive response to the trauma (e.g., I thought I might die), emotional distress (e.g., I was horrified by what happened) or physical symptoms (e.g., I had physical reactions like sweating, shaking, and pounding heart). The instruction for the PDI is to rate the extent to which each item was experienced “during the critical incident you selected and immediately after.” The PDI items are provided in the Supplementary Table 1. The total score is obtained by determining the mean response across all 13 items. The following factors were identified from the items of the PDI: Factor 1: Impotence/Inability to react; Factor 2: Sadness; Factor 3: Anger/Frustration; Factor 4: Loss of control; Factor 5: Fear; and Factor 6: Guilt and Shame. Administering the PDI to victims of domestic violence proved to be valuable in our investigation.
The Italian version of the PDI was used, which has demonstrated good test-retest reliability, convergent and divergent validity, and good internal consistency.19
2.1. Statistical analysis
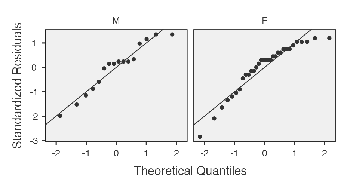
We used descriptives to provide a summary of the sample characteristics, including age, gender, and type of aggressor. We also used descriptives to summarize the scores of the Peritraumatic Distress Inventory (PDI) for both male and female victims. These statistics help to give a clear picture of the sample and provide a foundation for further analyses. Specifically, we used box plots, histogram plots, and scatter plots to describe the distribution of the sample based on both sex and PDI scores, while we used bar graphs to describe the frequency of all types of aggressors.
We used the Mann-Whitney U test to investigate whether female subjects had higher scores in the PDI compared to male subjects.20 We also used Shapiro-Wilk and Levene’s test to assess the normality and homogeneity of variance assumptions, respectively, required for the Mann-Whitney U test.21,22
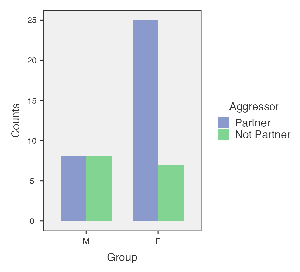
Furthermore, to investigate whether partners were the most frequent type of aggressor in our sample, we used contingency tables and the chi-square test.23 These statistical tests were employed to determine whether there was a significant association between the type of aggressor and the gender of the victim.
2.2. Ethical Considerations
This study adhered to the ethical principles of the Declaration of Helsinki and received approval from the Institutional Review Board of the University of Catania (protocol code 3-2018 of 18.06.2018). Written informed consent was obtained from all patients prior to the visit and the administration of the tools. The data and confidentiality of the participants were protected in the Catania Policlinico G. Rodolico, where we had an outpatient clinic and various archives. No personal or identifiable information was disclosed or shared with any third party. All data were anonymized and stored in encrypted files.
3. Results
Our study included 48 participants, comprising of 16 males and 32 females aged between 18 and 76 years (Table 1). The sample distribution was found to be non-normal. All participants had experienced physical domestic violence at the hands of someone living with them and sought medical attention at an emergency department. The age range for the male sample was 18 to 73 years, while for the female sample it was 21 to 76 years. The findings indicate that the male sample had a lower mean age (µ = 40.9) than the female sample (µ = 43.1) (Supplementary Figure 1; Supplementary Figure 2).
Based on our findings, it is apparent that the scores on the Likert-type scale in the female sample are significantly higher than those in the male sample. This implies that the female participants responded to the survey items with a high degree of agreement, with scores of 3 (very) or 4 (extremely true) (refer to Figure 1). This suggests that women who have suffered from domestic violence have experienced all the negative emotions assessed by the inventory, such as impotence/inability to react, sadness, anger/frustration, loss of control, fear, guilt, and shame. A more detailed analysis of the data shows that men primarily experienced feelings of sadness and anger/frustration.

We identified different types of aggressors in our study, and the Supplementary Table 2 shows that the husband (n = 14) was the most frequent aggressor against female subjects, followed by the domestic partner (n = 5), ex-husband (n = 3), and male son (n = 3). Among male subjects, the wife (n = 4) was the most frequent aggressor, followed by the ex-wife (n = 2), brother (n = 2), and other unspecified family members (n = 2) (Supplementary Table 3).
We also analyzed the frequency of aggressor types in our sample of men and women who reported experiencing domestic violence. Specifically, we tested whether partners were the most frequent type of aggressor (Table 3). The chi-square statistic for the analysis was 3.92, with a corresponding p-value of .048 (Supplementary Table 4). This indicates that the result is statistically significant at the .05 level, suggesting that partners are more likely to be the aggressors in instances of reported violence compared to other types of aggressors (Figure 2).

4. Discussion
The aim of this article is to analyse various types of aggressors and their victims in domestic violence situations and to compare the Peritraumatic Distress Index (PDI) scores obtained by women and men.
The article presents statistical analysis results obtained from data collected through a questionnaire administered to domestic violence victims. The results indicate that women are more frequently victimized by their husband, partner, ex-husband, and even by their male child; conversely, men are more frequently victimized by their wife, ex-wife, brother, and other unspecified family members. Furthermore, the results indicate that women have significantly higher PDI scores than men.
The study was conducted with methodological rigor, taking into consideration the heterogeneity of the data, and nonparametric tests appropriate for such data were employed. Specifically, the Shapiro-Wilk test was used to assess the normality of the data, while Levene’s test was used to evaluate the homogeneity of variances between groups. The article highlights the complexity of domestic violence and the significance of considering gender-related aspects in its analysis. It also underscores the importance of using suitable statistical methods for analysing non-normal data and assessing the homogeneity of variances between groups.
Research by psychologists has shown that Impotence/Inability to react, Sadness, Anger/Frustration, Loss of Control, Fear, Guilt, and Shame are common emotions experienced by individuals suffering from psychological trauma.24 These factors are analyzed in detail by the items of the PDI, the test used to assess the presence of a peritraumatic disorder. In addition to emotional factors, the cognitive response triggered by trauma is an essential factor leading to the emergence of peritraumatic distress and, consequently, PTSD. Feelings of fear and guilt can cause victims to engage in styles of cognitive maladaptive processing, such as rumination, as a way to cope with traumatic events, which can result in PTSD. On the other hand, a traumatic event can challenge an individual’s stable cognitive systems involving their understanding of the world.25 To build a post-traumatic understanding of the world, victims can re-examine their belief systems and reconstruct traumatic events, in which conscious or unconscious reflection on traumatic events plays an important role.26 Still, it is worth emphasizing that while maladaptive cognitive processing styles need to be unequivocally identified, victims support with clinical psychological interventions, such as time-limited group therapy, are also paramount.27 Clinical psychological interventions that are tailored for these situations, as well as those interventions that are trauma-informed, are likely to yield the best results. This evidence can be explained since trauma-focused clinical psychological treatments (including strategies to manage trauma-related symptoms) are particularly helpful for people who face continuous abuse or who are in shelter settings, leading to an increase in their sense of control over the situation and reducing symptoms of anxiety.28
4.1. Limitations
While this study offers valuable insights into the nature of domestic violence and the importance of considering gender aspects in its analysis, it is not without limitations.
The data were collected through a self-administered questionnaire, which may introduce response bias as the accuracy of the responses depends on the respondents’ honesty and their ability to accurately recall and report their experiences. Furthermore, the demographic characteristics of the respondents, such as their age, socioeconomic status, or cultural background, are not specified, making it unclear whether the findings can be generalized to other populations. The study used a cross-sectional design, which only captured a snapshot of a phenomenon at a particular point in time and does not allow for the examination of changes over time or the establishment of causal relationships. The lack of a control group for comparison could have provided additional insights into the effects of domestic violence. Lastly, domestic violence is often underreported due to fear, shame, or stigma associated with it, potentially leading to an underestimation of its true prevalence and impact. Despite these limitations, this study contributes significantly to our understanding of domestic violence and underscores the need for further research in this area.
5. Conclusion
Our findings revealed that female subjects reported higher scores on the Peritraumatic Distress Inventory compared to male subjects, suggesting that they experienced a greater level of peritraumatic distress in response to the traumatic events of violence. This finding highlights the importance of considering gender as a potential factor in the assessment and treatment of individuals who have experienced domestic violence.
Furthermore, our analysis showed that partners were the most frequent type of aggressors, supporting the notion that domestic violence is often perpetrated by intimate partners. This finding has important implications for the prevention and intervention strategies for domestic violence, highlighting the need for targeted clinical psychological interventions for couples and families.
In conclusion, our study sheds light on the psychological impact of domestic violence on victims and highlights the importance of considering gender and the type of aggressor in the assessment and treatment of individuals who have experienced domestic violence. These findings have significant implications for clinical practice and public policy aimed at reducing the prevalence and impact of domestic violence.
Author Contributions
P.C.: Conceptualization, Methodology, Software, Validation, Formal analysis, Investigation, Resources, Data Curation, Writing - Review & Editing, Visualization, Supervision, Project administration. V.L.: Conceptualization, Validation, Writing - Review & Editing. A.S.: Validation, Writing - Review & Editing. G.C.P.: Conceptualization, Methodology, Writing - Original Draft, Writing - Review & Editing. M.C.: Conceptualization, Methodology, Writing - Original Draft, Writing - Review & Editing. M.C.Q.: Resources, Writing - Review & Editing. All authors have read and agreed to the published version of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the University of Catania (protocol code 3-2018 of 18.06.2018).
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.