1. INTRODUCTION
A tumor is a pathological neoformation due to the more or less rapid proliferation of cells, which present the structure of the normal cells of the tissue from which they originate. When this is classified as malignant, it tends to spread rapidly both by local infiltration and by lymphatic and venous routes.1 Globally, the incidence of cancer rose to 18.1 million new cases and 9.6 million deaths (WHO 2018). By 2030, the number of new cancer cases will increase by 40% in high-income countries and by more than 80% in low-income countries. Cancer survival and mortality rates are also expected to increase with the number of long-term survivors.2 Brain tumours are clusters of abnormal cells in the tissues of the brain, which can be malignant or benign. It can affect parts of the brain or the spinal cord. The most frequent ones are gliomas, deriving from glial cells responsible for conducting essential functions, such as producing the myelin that lines the nerves of the nervous system. The Italian Association for Cancer Research (AIRC) reports that central nervous system tumors are quite rare and account for about 1.6% of all cancers. In 2020, 6,122 new cases were registered in Italy, more common in men (3,533 cases) than in women (2,589 cases) according to the data reported in the volume Cancer numbers in Italy 2020. Survival 5 years from diagnosis for this type of neoplasms remains low and is around 25%.2
Despite during awake surgery, neurosurgeons, in collaboration with neuropsychologists, have maximal safe resection as the modern goal for surgery of intrinsic brain tumors located in or close to brain eloquent areas,3 about 50% of cancer patients reported that, usually, specialists deal with physical rehabilitation and drug treatments, neglecting their emotional distress. This is where psycho-oncology comes in, which aims to promote the patient’s adaptation to treatment, emotional, psycho-physical well-being from a bio-psycho-social perspective.4
1.1. Psychological disease
In the following paragraphs we will discuss the most commonly encountered psychological disorders and cognitive deficits caused by a brain tumour.
1.1.1. Depressive Disorder
Psychological distress can occur in different forms on a continuum ranging from ‘normal’ fear, worry, or sadness to more severe clinical symptoms of anxiety, depression, and existential despair. In patients diagnosed with cancer, there is a 30-60% incidence of developing a mental disorder; the most frequent is depression.5
The most common symptoms are sleep difficulties, irritability, a tendency to cry, overcoming pain not compatible with the medical condition, disability and dependence on structures or people, the loss of one’s body image, progressive environmental and social isolation, and death.6 Loss of hope, accompanied by despair, can be more of a symptom of depressive disorder. Furthermore, patients can feel guilty about their family members, feeling like a burden, causing them serious inconvenience and suffering.7
1.1.2. Anxiety disorder
Pain, hypoxia, endocrine disruption, discontinuation of drugs, surgical treatments, chemotherapy, radiotherapy, and news of a recurrence can develop into anxious symptoms, even to the point of developing serious anxiety disorders. Symptoms are divided into psychic and somatic, with the former being feelings of anxiety, apprehension, fear, anticipation of danger, restlessness, impatience, fatigability, distractibility, and difficulty concentrating. Somatic symptoms are tachycardia, increased blood pressure, increased muscle vascularity, sweating, dry mouth, dizziness, chest tightness and air hunger, and gastrointestinal disturbances (nausea, vomiting, diarrhoea).6 In addition to common anxiety syndromes such as panic disorder or phobias, post-traumatic stress disorder and anticipatory nausea and vomiting disorder are often found. Phobias, usually called simple phobias, are defined as a disproportionate reaction to specific stimuli or objects, such as in this case phobias of syringes, of the hospital.4
1.1.3. Post-traumatic stress disorder
Cancer can lead to a sense of loss of control and helplessness in the patient receiving the diagnosis. It is an event that weighs heavily on the life of the subject in question; it can be chronic and lethal, perceived as a threat to physical and mental health, often painful, and with side effects. So, researchers and professionals believe it is legitimate for the patient to experience cancer as a traumatizing experience, up to the possible development of post-traumatic stress disorder.7
1.1.4. Delirium
The APA recognises delirium as a neuropsychiatric syndrome, characterised by a brain deficit with acute onset and fluctuating course. It can be characterised by the presence of a deficit in attention and perception of the environment, disorganised thinking, altered level of consciousness, cognitive disturbances such as spatial time disorientation and memory deficits, hallucinations, impairment of abstract thinking and comprehension, altered speech, delusions, altered sleep-wake cycle, and altered psychomotor activity.6 Chemotherapy and immunological therapy with cytokines can cause irreversible and acute toxicity of the central nervous system. Scientists argue that symptoms attributable to interferon, interleukin 2 (IL-2) and tumor necrosis factor (TNF) can cause the typical symptoms of delirium, especially in hospitalized cancer patients.4
1.1.5. Cognitive Disorders
Based on the location of the tumor mass and subsequently acquired injuries (ABI), cognitive abilities can be impaired with progressive cognitive decline.8 Then higher brain functions are compromised: attention, perception, thinking, reasoning, and remembering; motor and language skills are also impaired. Radiation therapy can lead to focal deficits, such as neural necrosis, encephalopathy, and dementia.9 Anderson et al. state that brain tumour patients are less likely to experience a language disorder than stroke patients.10 Usually, Broca’s and Wernicke’s areas are not affected by a neoplasm, unlike stroke, suggesting that language function depends on a set of cognitive abilities, so that a wider network of cortical regions is involved. Deficits in these areas, due to tumour lesions, lead to aphasia, semantic dementia, anomic aphasia, conduction aphasia, non-fluent aphasia and apraxia of speech.11 Zucchella et al.12 described three clinical cases at the Mediterranean Neurological Institute with cognitive deficits due to primary neoplasm treated surgically. The patients reported nominum aphasia, memory disorders, logic-attentive deficits and ideomotor slowing.
In recent years, an increasing number of studies have highlighted the usefulness of reliable preoperative planning based on noninvasive techniques to define the best customized surgical approach for gliomas in eloquent areas,13,14 but although the cognitive functioning remains intact, this allows the patient to function autonomously within the society, therefore, in the case of primary or metastatic brain tumors, it is important that the functioning is preserved and improved. Maintaining and enhancing a patient’s cognitive abilities can contribute to their overall well-being during their illness. This is because cognitive functions, such as memory, attention, and problem-solving, are essential for daily living and independence. When these functions are preserved, patients can continue to engage in their usual activities and social interactions, which can improve their quality of life and emotional well-being during their treatment journey.4 One of the innovative surgical methods for tumor removal is awake surgery with intraoperative electrical stimulation and real-time monitoring, to preserve language and motor function.15 The most common psychological interventions in the oncology field are counselling in a hospital setting and psychotherapy. Psychological counselling is typically followed in hospital wards and follows a specific process.4
1.1.6. Evidence-based Psychological Treatments
Cancer disrupts each patient’s sense of life, changes the body and the mind. The nosographic manuals do not give precise indications on psycho-oncological disorders: related symptoms are either secondary or ‘need further study’, due to the breadth of individual problems found in patients. From the clinical point of view, psychotherapeutic interventions are not directed towards the pathology, but, essentially, towards the patient’s emotional and relational distress that accompanies the illness.4 Psychotherapeutic treatments can be of different orientations, but in general, research shows that they allow for a decrease in anxiety, depression, and chronic pain. The common aim is preventing or reducing the reported psychopathological disorders. For example, Cognitive Behavioural Therapy (CBT) is a psychotherapeutic approach that emphasizes the significance of how our thinking affects the way we feel.16 In recent years, it has also been used for to treat pain caused by various oncological and hematological disorders.17
There are several techniques in the literature: Compen et al. proposed Mindfulness-based cognitive therapy (MBCT) with the help of the Internet (eMBCT) to relieve distress in cancer patients, comparing MBCT and eMBCT versus TAU (treatment as usual).18 The eMBCT was delivered individually and involved weekly asynchronous written interaction with a therapist via e-mail. Each session included an introduction and daily meditation exercises with meditation audio files. In the off-day week, patients were provided with a schedule like the MBCT rest day. These interventions demonstrated similar reductions in fear of cancer recurrence, brooding, mental improvements, health-related quality of life, mindfulness skills, and positive mental health.
Another method is neurofeedback, which aims to guide the brain towards generating brain waves with more functional amplitude and frequency. It involves teaching individuals how to self-regulate their brain activity through learning and operant conditioning techniques.4 In a case study, Lagravinese et al.19 reported the effectiveness of neurofeedback (NFB) for the treatment of acquired cognitive impairment after surgery for a brain tumor in a woman with tubercle meningioma of the sella. After the NFB training sessions, she showed an improvement in executive and functional functions. At the end of the rehabilitation cycle, she successfully recovered mobility, balance, and motor autonomy.
Furthermore, a recent review by Caponnetto et al.20 aimed to understand how modern technologies can be integrated with psychological approaches. Virtual Reality is increasingly being recognized as a valuable tool in treating conditions like depression and anxiety. From these results, the aim is to demonstrate how virtual reality and new technologies can be a valuable aid for cancer patients in the treatment of the psychophysical disorders that characterise the disease.
2. METHODS
2.1. Research Goal
The aim of this research is to systematically review the literature on interventions for mental distress in patients diagnosed with cancer and to detect innovative intervention strategies to treat the neuropsychological consequences. Our decision to concentrate on patients with brain cancer stems from the limited number of comprehensive studies available in the literature for this cancer type. The second reason is to provide researchers with a clear framework for future research to fill the gaps in the literature by providing new treatments, also considering new technologies, that can improve patients’ quality of life by reducing or preventing possible psychological disorders.
2.2. Search Strategies
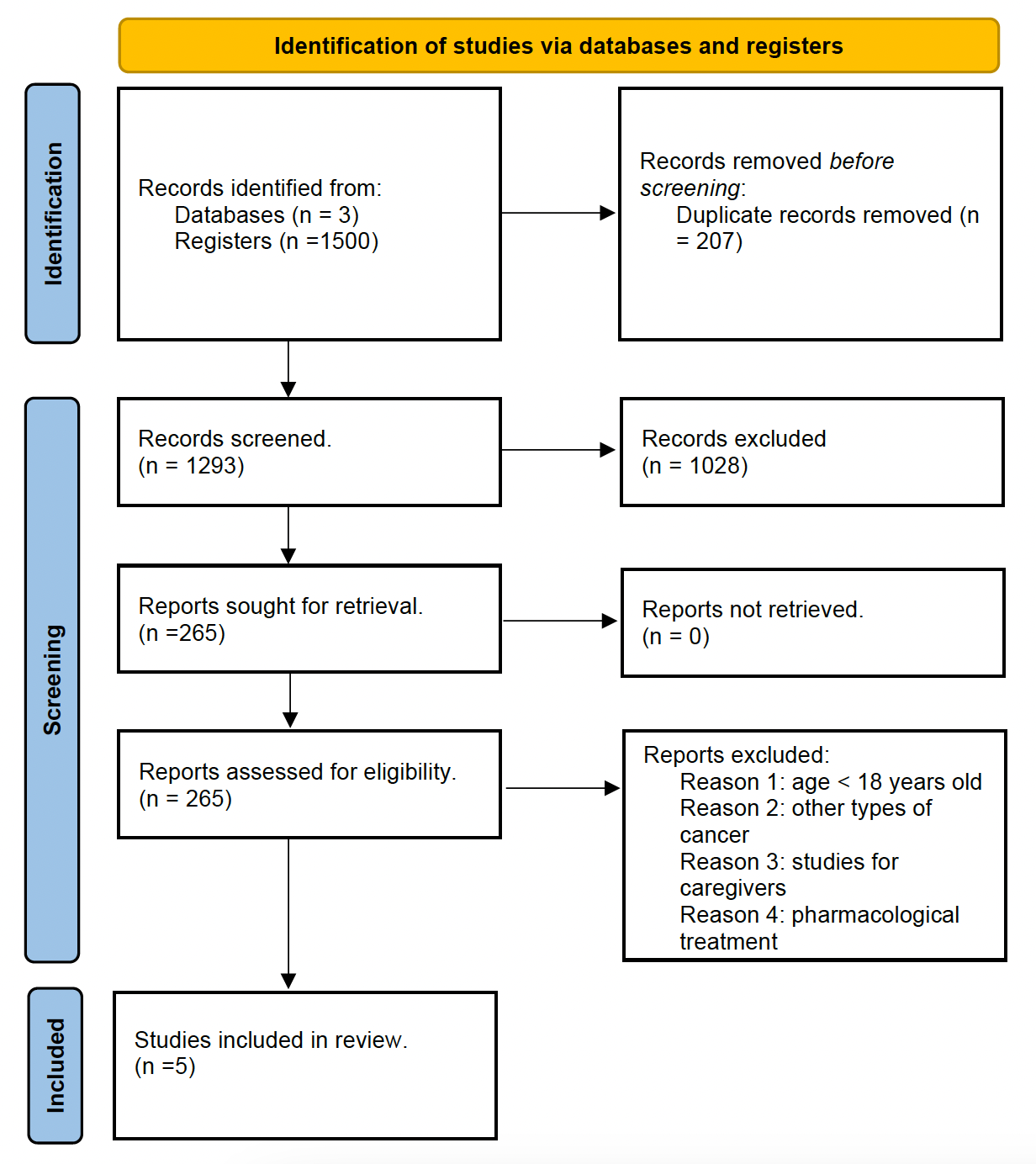
This systematic review has been completely carried out according to the PRISMA 2020 guidelines for the systematic revision of the PRISMA Group21 (Figure 1). The literature search was carried out from February 2022 to 31 December 2022 in the databases of PubMed, PsycNet, and Web of Science using the following string of search terms: “psychological implications and brain cancer” OR “psychiatric and psychosocial implications and cancer” OR “neuropsychology and brain cancer” OR “treatment and cancer” or “psychotherapy and cancer” OR “CBT and brain cancer” OR “cyberpsychology and cancer”.

2.3. Eligibility Criteria
We included every article written in English with no time limit to the date of publication, meeting the following criteria (PICO framework):
-
Participants: adults with cancer and mostly adults with and after brain cancer.
-
Intervention: cancer patients must have been treated with classical CBT rehabilitation.
-
Comparison: some research had to compare psychological interventions and cognitive rehabilitation, from classic cognitive-behavioural therapy or classical therapies to new technologies.
-
Outcomes: regarding the results, the presence of psychological implications and cognitive deficits was taken into consideration in an attempt to identify specific and innovative treatments.
2.4. Exclusion Criteria
We excluded all studies involving the paediatric population, those that sampled caregivers, studies with pharmacological or organ-only treatments. We did not report case studies or studies in textbooks. We have excluded certain forms of psychotherapy, for the sole purpose of reporting evidence-based data.
2.5. Data Extraction
Through the databases, we found a total of 1500 studies. Of those excluded were 207, they were duplicated. We included studies by reading titles and abstracts up to 265. We included studies that dealt with psycho-oncology, all of which dealt with psychological and cognitive deficits in adult patients (over 18 years of age) with cancer, and in particular brain cancer. Among the inclusion criteria, we considered only studies with treatments aimed at neuro-oncological patients (Table 1).
Risk Of Bias Assessment
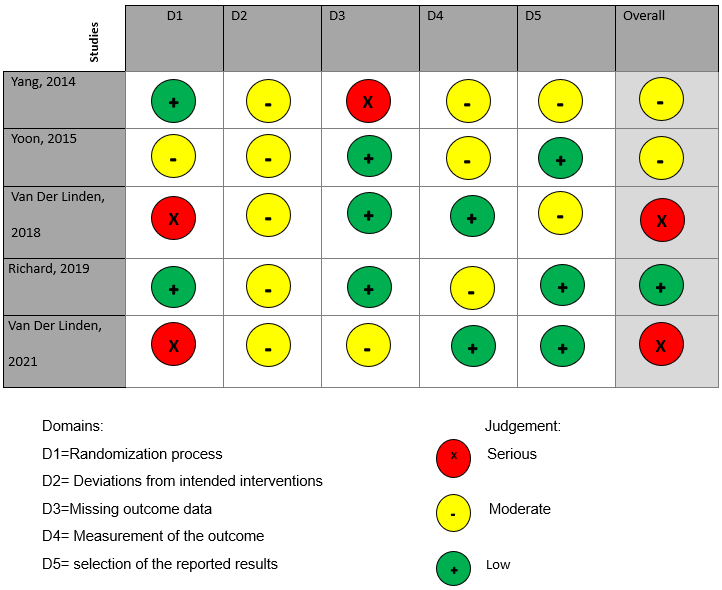
For the different studies, we performed an assessment of the possible risks of error. We have considered the possible risks of error related to the randomization processes, the deviations from intended interventions, the missing outcome data, the measurement of the outcome, the selection of the reported results, and overall (Figure 2). The risk of bias for the included studies was assessed with Cochrane risk-of-bias tool for randomized trials, version 2 (RoB 2).22

3. RESULTS
3.1. Characteristics Of the Included Studies
In this paragraph we present the characteristics of the studies that we have analysed, focusing on the treatments used by the researchers.
3.1.1. Cognitive Behavioural Treatment
Richard’s pilot study on cognitive rehabilitation in patients with brain tumors using a behavioural treatment aimed to assess cognitive functions in neuro-oncology patients, particularly attention, memory, and behavioural disorders, so that they could be relied upon for cognitive rehabilitation.23 They evaluated the effectiveness of Goal Management Training (GMT), a program using both mindfulness and strategy training, compared with an innovative psychoeducational program, the Brain Health Program (BHP), and a wait-listed control group (WAIT). The sample consisted of 25 patients, all survivors of a primary brain tumor and randomly divided among the three types of treatment. Although no significant baseline differences were found between GMT, BHP, and WAIT in demographics, disease, and treatment, the results reported cognitive improvements with the GMT programs, significantly improving their daily lives. A small and moderate improvement in evaluative function was shown in GMT and BHP, while in WAIT, emotional functioning improved slightly from onset to follow-up. After training, all BHP and GMT patients reported using the knowledge and tools of their programs at least 2-3 times per week, with actual applications more frequent in the GMT. In summary, this study suggests an improvement in the management of cognitive problems in neuro-oncology patients using the proposed clinical methods.
3.1.2. New technologies
Van Der Linden et al. (2018) through their randomized trial demonstrated how effective the cognitive telerehabilitation program, using an app on the iPad- ReMind that includes psychoeducation, strategy training, and retraining.24 The participants were 13 patients (38 percent female), with an average age of 52 years (range 40-68), who have followed the cognitive rehabilitation program and completed all assessments. ReMind provided six modules, specifically on: Cognitive Functions, Influences, Compensation, Attention, Planning and Control, and Memory. In the retraining portion, called C-Car, four different attention modes, namely sustained, selective, alternating, and divided attention. It included visual and auditory exercises, in which both verbal and numerical stimuli are presented. During the intervention period, the researcher contacted the patients by phone every two weeks to check on their progress, plan the course of their training, and ask questions. It was recommended and planned that patients spend 3 hours per week in the program, to complete it within 10 weeks. At the end of these, a second face-to-face appointment was held to retrieve the iPad and collect the completed questionnaires. After completing the program, all participants indicated that they would recommend the program to other brain tumor patients. Cognitive rehabilitation such as this described allows many brain tumor patients to follow a program at home, which is a great advantage since many patients cannot drive because of seizures. Another important advantage is that the patients can follow the program at their own pace and can distribute the material over as many sessions as they want, which could be especially useful for vulnerable patients and the elderly.
Three years later (2021), the same research group conducted a further study on eHealth cognitive rehabilitation for brain tumor patients.25 This randomized controlled trial aimed to evaluate the effects of a tablet-based cognitive rehabilitation program called ReMind on cognitive performance, cognitive complaints, fatigue, and psychological distress in primary brain tumor patients following neurosurgery. The study also assessed attrition, adherence, and patient satisfaction with the program. Adults with presumed low-grade glioma and meningioma were recruited before surgery. Three months after surgery, participants were allocated to either the intervention group or a waiting-list control group. The 10-week eHealth app ReMind, based on an effective face-to-face intervention, consisted of psychoeducation, strategy-training, and attention retraining. Cognitive outcomes and patient-reported outcomes were assessed before surgery and at 3, 6, and 12 months after surgery. The study compared mean scores, percentages of cognitively impaired individuals, and reliable change indices (RCIs) between groups. Out of 183 eligible patients, 62 were randomized. Of those who declined, 56% reported that participation would be too burdensome. All participants found a tablet-app suitable for delivering cognitive rehabilitation, and 90% rated the program as “good” or “excellent.” However, there were no significant differences in performance-based cognitive outcomes and patient-reported outcomes in group means over time or RCIs between the intervention (final n = 20) and control group (final n = 25). The study concluded that recruitment at this early stage was difficult, resulting in limited statistical power. Although no significant effects were demonstrated, adherence and satisfaction with the eHealth program were good. In clinical practice, ReMind may be helpful if the timing is adapted to patients’ needs.
3.1.3. Virtual Reality
We included two studies on the use of virtual reality in the treatment of brain cancer patients. The study of Yoon et al. (2015)26 aimed to evaluate the benefits of virtual reality-based rehabilitation (VRBR) on upper-extremity function in patients with brain tumors. Patients with upper-extremity dysfunction were divided into two age-matched and tumor type-matched groups. The intervention group underwent a virtual reality program for 30 minutes per session for 9 sessions and conventional occupational therapy for 30 minutes per session for 6 sessions over 3 weeks. The control group received conventional occupational therapy alone for 30 minutes per session for 15 sessions over 3 weeks. Various tests were used to evaluate upper-extremity function, such as the Box and Block test, the Manual Function test, and the Fugl-Meyer scale. The Korean version of the Modified Barthel Index was used to assess activities of daily living. Results showed that both groups exhibited significant posttreatment improvements in all test scores. However, the intervention group demonstrated greater improvements in shoulder, elbow, and forearm function, while the control group showed better hand function. The study concluded that VRBR combined with conventional occupational therapy may be more effective than conventional occupational therapy alone, particularly for proximal upper-extremity function in patients with brain tumors. Further research is needed to explore virtual reality programs targeting hand function.
The second study is by Yang et al.(2014)27 was performed on 38 brain tumor patients (19 men and 19 women) with cognitive impairment, using Virtual Reality. The VR programs consist of a three-dimensional, real-time environment that allows patients to participate in real-time situations. All the patients included reported cognitive impairment. Nineteen patients were assigned to the VR group with IREX, with a mean age of 48 years and 19 to the control group with an age of 53 years. The program of attention consisted of three courses at beginner, intermediate and advanced levels. The activities were attention training, attention discrimination, visual perception, auditory perception, continuous attention, integration of attention, and the one on emotions. The level of training was determined according to the difficulty of the task and the condition of the patient. For memory, the program was divided into three levels of difficulty and included simple spatial memory training, simple recognition memory of: sequential recall, sequential verbal recall, associated recall memory, verbal categorization, and integrated memory training. Patients were assigned verbal/non-verbal tasks and sequential/non-sequential tasks. VR can be useful for patients with brain malignancy, especially with the consequence of cognitive impairment.
4. DISCUSSION
This systematic review focuses on the critical need for effective interventions to alleviate mental distress in brain cancer patients. While there is a growing body of literature on cancer-related mental health, there is a significant research gap when it comes to specifically targeting individuals with brain cancer. These patients encounter unique neuropsychological and psychological challenges due to the nature of their condition. Our research systematically reviewed existing literature on intervention strategies for mental distress in cancer patients, with a particular emphasis on identifying innovative approaches that can enhance their quality of life. In our exploration of the psychological and cognitive implications for neuro-oncology patients, we have chosen to consider studies that employ a cognitive-behavioral approach, combined with cognitive rehabilitation techniques. Our goal was to identify interventions that can enhance patients’ quality of life by targeting executive functions, which are crucial for daily living.
Following the chronological order of the table 1, in the first two studies, the authors demonstrated the effectiveness of virtual reality in cognitive27 and motor26 rehabilitation in brain tumour patients. In Yoon’s et al. study (2015), there were statistically significant improvements in the recovery of shoulder, elbow and forearm movement using conventional occupational therapy combined with virtual reality programs. Although the results of the improvement in quality of life were similar in the intervention and control group, they already supported the usefulness of using virtual reality in the functional recovery of patients’ movement.26 Yang et al. (2014) had also highlighted the effectiveness of VR, which allowed patients with cancer patients the recovery of impaired functions through the performance of different tasks.27 In both studies, virtual reality was used with IREX and the same programs (Conveyor, Coconuts, Bird and Balls, Football, Jugger) plus one added (Dumbs) in Yoon’s study.26 Yang emphasized the motivation of patients to participate in these types of interventions, which are certainly innovative and active, so that effective rehabilitation after cancer treatment can be designed.27
In the third study, Van der Linden et al. wanted to highlight how new technologies can be used in psycho-oncology rehabilitation. In the 2018, Van der Linden et al.24 investigated the feasibility of the Remind app, for the rehabilitation of cognitive functions, influences, compensation, attention, planning, control, and memory. Positive feedback from participating patients, who recommended this remote rehabilitation approach to others, led to a subsequent randomized controlled trial in 2021 (fifth study)25 using the same tablet based Remind app. An important point was made in this last study: many patients who leave rehabilitation claim that they prefer to spend more time at home, with their family. Thus, although the methods prove to be cognitively effective, the needs of cancer patients should not be neglected. The authors, therefore, emphasize the importance of developing programs that can be conducted remotely, so that patients can devote themselves both to their relationships and fully adhere to rehabilitation strategies.25 In support of these aforementioned studies by Van der Linden et al., a pilot study by Taylor et al.28 examined the feasibility and efficacy of three cognitive rehabilitation strategies for patients with stable lower grade gliomas (LrGG): in-person rehabilitation, an iPad-based program (ReMind), and daily instructional text messages (Healthy SMS). Out of 60 patients, 23 participated in the study. The most common cognitive impairment was processing speed. Feasibility results showed 71% for in-person rehabilitation, 50% for ReMind, and 100% for Healthy SMS. Preliminary findings suggest that stable LrGG patients can engage in cognitive rehabilitation interventions.
In the fourth study,23 Richard et al. wanted to test the effectiveness of GMT in improving the executive dysfunction in brain tumor cases, compared with BHP and WAIT, reporting that the former two reported improvements in global, attentional, and amnestic functions in patients with brain tumors. A study by Krasny-Pacini et al.29 had already demonstrated a few years earlier the effectiveness of Goal Management Training (GMT) for rehabilitating executive functions following brain injury, either alone or in combination with other interventions. The study found that GMT was more effective when combined with other interventions, such as Problem Solving Therapy, personal goal setting, external cueing or prompting, personal homework, and ecological and daily life training activities. The study also found that comprehensive rehabilitation programs incorporating GMT, but integrating other approaches, are effective in executive function rehabilitation following brain injury in adults. Recent studies, such as the one conducted in 2021 by Egset et al.,30 have shown that GMT can be used for cognitive rehabilitation of survivors. In fact, they conducted the first study to explore the feasibility of GMT for adult survivors of childhood Acute Lymphoblastic Leukemia (ALL). The study found that the GMT protocol is feasible and acceptable for ALL survivors, despite high levels of fatigue and relatively low Health-Related Quality of Life (HRQoL). Moreover, the study also suggests that GMT may have the potential to produce reliable improvements in daily life Executive Functioning (EF) and neurocognitive functioning for adult ALL survivors with long-term late effects. GMT is effective in brain tumour survivors with clinical stability and can be an effective approach for the management of deficits in neuro-oncology. However, new technologies are proving to be more advantageous for these types of patients. In fact, in a recent review conducted by Van Lonkhuizen et al. (2019)31 the main intervention techniques for cognitive problems of adults with brain cancer are investigated: again, how different techniques can improve cognitive aspects in oncology patients are demonstrated, influencing their feelings for a better recovery of their lives after a diagnosis of trauma, such as that of brain cancer. The authors also referred to articles demonstrating the usefulness of new technologies.
4.1. Clinical Implications
This systematic review underscores the urgent for need effective interventions to alleviate mental distress in patients with brain cancer. These patients face unique neuropsychological and psychological challenges due to the nature of their condition, and there is a significant research gap in targeting this specific population. Our research has systematically reviewed existing literature on intervention strategies for mental distress in cancer patients, with a particular emphasis on identifying innovative approaches that can enhance their quality of life. We considered studies that employ a cognitive-behavioral approach, combined with cognitive rehabilitation techniques. Our objective is to identify interventions that specifically target executive functions, which play a crucial role in the activities of daily living. In this way, it is possible emphasize the potential of novel strategies, such as virtual reality and mobile apps, in improving the quality of life for individuals with brain cancer. These interventions can target crucial cognitive functions and can be tailored to the needs and preferences of the patients. However, more research is needed to further explore these interventions and to address the significant research gap in this area.
4.2. Study limitations
Although the results of the above-mentioned studies showed promise for designing new rehabilitation programs, there are many limitations found: the psychophysical aspects in patients are subjective so that they do not have precise frameworks; the treatments are not specific, therefore, various psychological approaches and techniques are adapted according to related psychological symptoms and reported deficits; in the literature, the greatest research focuses on breast, lung, colorectal and chronic pain, so few focused on the emotional and social disruptions of brain cancer. This aspect, therefore, also falls on the treatments that, although valid in the cognitive sphere, are in lesser number on the emotional and psychological aspects.
5. CONCLUSIONS
This systematic review showed how neuropsychology treatments can benefit a person’s psychophysical recovery, especially in contexts of brain oncology. Some intervention techniques can enable the patient to recover most of his/her executive and cognitive functions: the patient can continue to reason, talk, move, and listen, even with the consequences that a brain neoplasm can bring. By concentrating on this underserved population, we hope to contribute to a better understanding of their needs and develop tailored interventions that can reduce or prevent psychological disorders following a traumatic event. Finally, although the limitations present today, future studies should focus on various psych-rehabilitation treatments to improve their quality of life, becoming increasingly targeted and including the help of new technologies that are increasingly relevant.
FUNDING INFORMATION
This research received no external funding.
AUTHOR CONTRIBUTIONS
Conceptualization, M.M., G.S., P.C.; methodology, P.C.; resources: G.S.; data curation: G.S.; writing—original draft preparation, G.S.; writing—review and editing, G.S., M.M., P.C., G.C.P. and C.B.; supervision, M.M., C.B., M.C.Q. and P.C.; All authors have read and agreed to the published version of the manuscript.
ACKNOWLEDGEMENTS
Thanks to all the authors for their participation and careful supervision in the drafting of this work.
CONFLICT OF INTEREST
The authors declare no conflict of interest.