

Introduction
Almost every 39 seconds, an American will have a heart attack and every year, about 605,000 people in the United States die from one.1 Even though this is one of the leading causes of death, the level of knowledge among the lay public has consistently been demonstrated to be poor. A study conducted in Victoria, Australia demonstrated that although 84.6% of respondents reported chest pain as being a symptom of a heart attack, only 4.2% were able to identify at least five correct symptoms.2 A study of 3,051 Chinese adults showed that on average, participants recognized 5.2 out of 14 stroke symptoms and 2.6 out of 6 heart attack symptoms, but did not recognize less typical symptoms like nausea and a feeling of anxiety3 as being potential signs of a heart attack. A study of laypersons in Thailand concluded that older adults knew less about heart attack symptoms when compared to their younger counterparts, irrespective of gender or educational differences.4 A telephone survey of over 1800 New York City residents found that women were significantly more likely than men to know that sex differences exist in the warning signs for a myocardial infarction (MI) and that Whites had above-average confidence in MI recognition and pubic AED availability compared with non-whites.5 The value of educating the general public on the basic knowledge of heart attack symptoms is so that people would be able to easily recognize the symptoms earlier on which could save lives. Giving people this knowledge allows them to not solely depend on medical care which ends up in delays in seeking medical care. These delays could cause deaths that potentially could be avoided.
Methods
Two hundred Georgia residents were surveyed about their general knowledge on heart attacks via an online survey platform. De-identified data obtained for analysis. There was no specific target population, the only specifier was that the responder must be a resident of Georgia. The software used to analyze the data was JMP (Version 16). The significance threshold was alpha = .05 and all confidence intervals were 95%. The study was deemed exempt by our institutional review board, study # 2022-1103.
Results
The cohort was 44% female. The racial distribution was 27% Black, 60% White, 4% Hispanic, 2% Asian and the remainder were mixed or preferred to to say. Thirty four percent were married. 11% were living with their partner, 7% were divorced, 3% were separated, 3% were widowed, and 38% were single.
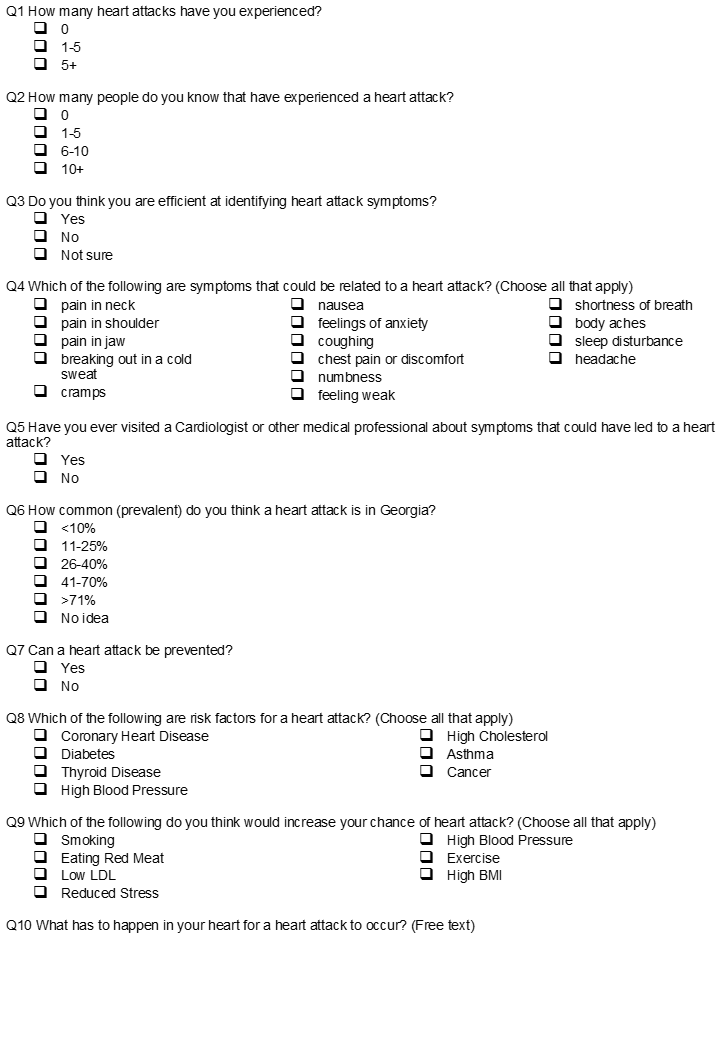
The survey consisted of 10 questions (figure 1) that asked about general heart attack knowledge such as symptoms and personal history. Eighty five percent of respondents had 0-5 heart attacks, while the other 15% responded 5 or more. Seventy percent said they knew 5-10 people who had had a heart attack, 20% said they knew 0-5 people and 8% responded 10+. When asked if they thought that they were proficient in responding accurately to questions related to heart attack and 50% said yes, 23% said no, and 27% said maybe.

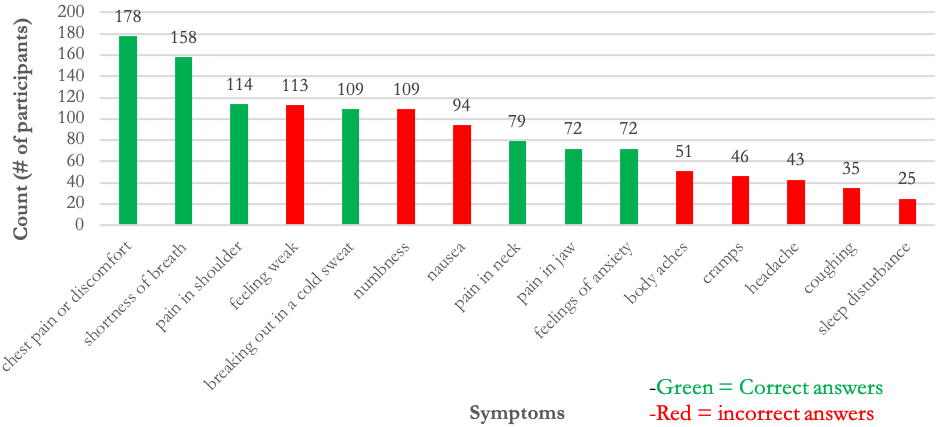
When asked to pick as many symptoms from a list of heart attacks symptoms that they thought were related to a heart attack, the responses were varied (Figure 2).

When asked if they had ever visited a cardiologist or any other medical professional about symptoms that could have led to a heart attack, only 28% said yes. When asked how common a heart attack was in Georgia, 5% said 10% and lower, 20% said 11-25%, 36% said 26-40%, 16% said 41-70%, 7% said 71% and greater, and 16% said that they had no idea. Ninety one percent thought a heart attacked could be prevented. When asked what the main cause of a heart attack is, 80% were able to pick out coronary heart disease, but fewer could identify diabetes, thyroid disease or high blood pressure (figure 3) as risk factors.

When asked what would increase your chance of a heart attack, 85% said smoking, 46% said eating red meat, 12% said high cholesterol, 8% said reduced stress, 90% said high blood pressure, 8% said exercise, and 66% said high basal metabolic index. The final question was an open-ended one in which respondents were asked what they thought had to happen in the heart for a heart attack to occur. Only 24% of the written responses were correct, with most stating they didn’t know (figure 4).

Discussion
The data shows us that Georgians have a limited understanding of heart attacks. Georgians were able to identify some aspects of heart attacks such as the major risk factor of heart attacks which was coronary heart disease. A majority (91%)were also able to identify that a heart attack could be prevented. A majority (90%) also said that high blood pressure would increase your chance of a heart attack. Surprisingly, 72% of people did not visit a cardiologist or any medical professional about symptoms that could have led to a heart attack. More than 50% felt that shoulder pain was not a symptom of a heart attack. Health literacy represents a person’s ability to access and use knowledge, resources, and organizational structures to promote and maintain good health.6 This can be summarized as health literacy and social determinants of health contributing to improved health outcomes.7 A study of over 500 adults in the Southern Unites States found that health literacy was significantly associated with health seeking behavior.8 Health literacy is strongly correlated with overall literacy and numeracy. Georgia residents, where the state literacy rate is only 76.4%,9 makes it the 10th most illiterate state. Correspondingly, Georgia also ranks as the 10th poorest state in the US. These facts would suggest that laypersons in Georgia are not well prepared to handle a cardiovascular emergency.
Limitations
While online survey research has numerous advantages including ease of administration, speed with which responses can be gathered, and low cost, it also has important limitations.10 As with any data collection method, the data analysis is only as good as the data inputted. In the current paper, the online survey method relies on the respondent being able to read, and utilize technology (smart phone).11 This may in fact have inadvertently excluded many Georgia residents. These would lead to sampling bias. Respondents may also answer without much thought or intention in order to get through the survey faster as the online platform also decreases accountability. This would lead to response bias.12
Conclusion
This cross-sectional survey of Georgia residents demonstrates
limited understanding of heart attacks. Improved health literacy is
imperative to improve knowledge and hopefully translate to
improved morbidity.