




Introduction
Dysmenorrhea describes painful uterine contractions during menstruation. It is widely regarded as the most common gynecological disturbance with varying estimates in prevalence. While one systematic review of chronic pelvic pain reports symptoms of dysmenorrhea in 16.8% to 81% of menstruating women, another paper suggests this number is between 45% to 95%.1,2 In addition to cramps, women with dysmenorrhea may experience gastrointestinal symptoms, such as nausea, vomiting, diarrhea, bloating, or constipation. Collectively, these symptoms limit women’s ability to participate in social, academic, occupational, and sports activities. Despite these effects on quality-of-life, most women report not consulting a physician due to a belief that visiting an expert would not help.2
There are two categories to classify a patient’s dysmenorrhea. Primary dysmenorrhea describes menstrual pain without an associated condition while secondary dysmenorrhea is related to an underlying cause. Onset begins 6 to 12 months after menarche with the highest frequency occurring in one’s late teens or early twenties.3 Secondary dysmenorrhea occurs most often due to endometriosis but may also be caused by fibroids, adenomyosis, endometrial polyps, or the use of an intrauterine contraceptive instrument. Compared to white women, it has been found that black women have a 40% lower incidence of endometriosis.4 Patients reporting more severe cramps are likely to have higher levels of uterine prostaglandins.2
In this study, the authors aimed to measure the prevalence of dysmenorrhea, its impact on quality-of-life, and the relationship between income and access to oral contraceptive pills (OCP) in a sample of 200 eligible participants.
Methods
Recruitment and Data Collection
Two hundred women (n=200) from the United States (US) were administered a questionnaire with queries related to menstruation. This questionnaire was made available to participants using a survey research platform that uses organic sampling based on random device engagement (RDE). Through the platform’s integrated algorithms, single users on multiple accounts are excluded to ensure each response represents a unique individual participating in the study. To be considered eligible for the study, participants were required to be female and at least 16 years of age. In addition to responses from the survey questions, additional demographic information pertaining to age, gender, education, income, and race was also collected. The survey had 15 total questions. The first two asked respondents to quantify their menstrual pain and flow from 1 (lowest) to 5 (highest). The next question asked about which symptoms participants experience during their period. Eight questions were then given to ask about any activities that were missed due to painful menstruation and for the amount of time. The remaining questions polled medications, birth control, or any other remedies that help the patient cope with pain. Most questions were multiple choice with only one response allowed except for question three, which permitted several answers, and the final question, which was open-ended. This survey study did not involve a power analysis or planning (ad hoc) for a specific minimum sample size.
Statistical Analysis
All data collected from the survey was analyzed using JMP. The significance threshold was alpha = 0.05 and all confidence intervals were 95%.
Results
Our cohort’s age ranged from 17 to 79 years. The interquartile age was 30.3 to 50 years, with the median age being 38.5 years old. 51.5% of the cohort had zero children, 15.5% had one, 17% had two, 6.5% had three, 6% had four, 0.5% had five, 2% had six or more, and 1% preferred not to say. The marital status of survey participants was as follows: 5% of the cohort was divorced, 17% were living with their partner, 32.5% were married, 3% were separated, 38% were single, 4% were widowed, and 0.5% preferred not to say. By race, 66% of the cohort was white, 2.5% was Asian, 11% was black/African/African American, 10.5% was Hispanic, 4.5% was Latino, 2% was multiracial, 1% was other, and 2.5% preferred not to say. Participant income level was self-reported using the following system: high iii (5%), high ii (3.5%), high i (7.5%), middle ii (10%), middle i (15.5%), lower ii (28%), and lower i (27%). These coded tiers correspond to the following earning levels per year: high iii over $150,000, high ii between $125,000 and $149,999, high i between $100,000 and $124,999, middle ii between $75,000 and $99,000, middle i between $50,000 and $74,999, lower ii between $25,000 and $49,999, and lower i less than $24,999.
How would you rate the pain from menstrual cramps on a scale of 1 (not painful) to 5 (extremely painful)?
7.0% of the cohort responded 1 or not painful, 9.0% responded 2 or a little painful, 31.5% responded 3 or somewhere in the middle and somewhat painful, 35.0% responded 4 or painful, and 17.5% responded 5 or extremely painful (Fig 1).

How would you rate your menstrual flow on a scale from 1 (very light) to 5 (very heavy)?
9.5% of the cohort responded 1 or very light, 3.5% responded 2 or light, 42.5% responded 3 or medium, 27.5% responded 4 or heavy, and 17.0% responded 5 or very heavy (Fig. 2).

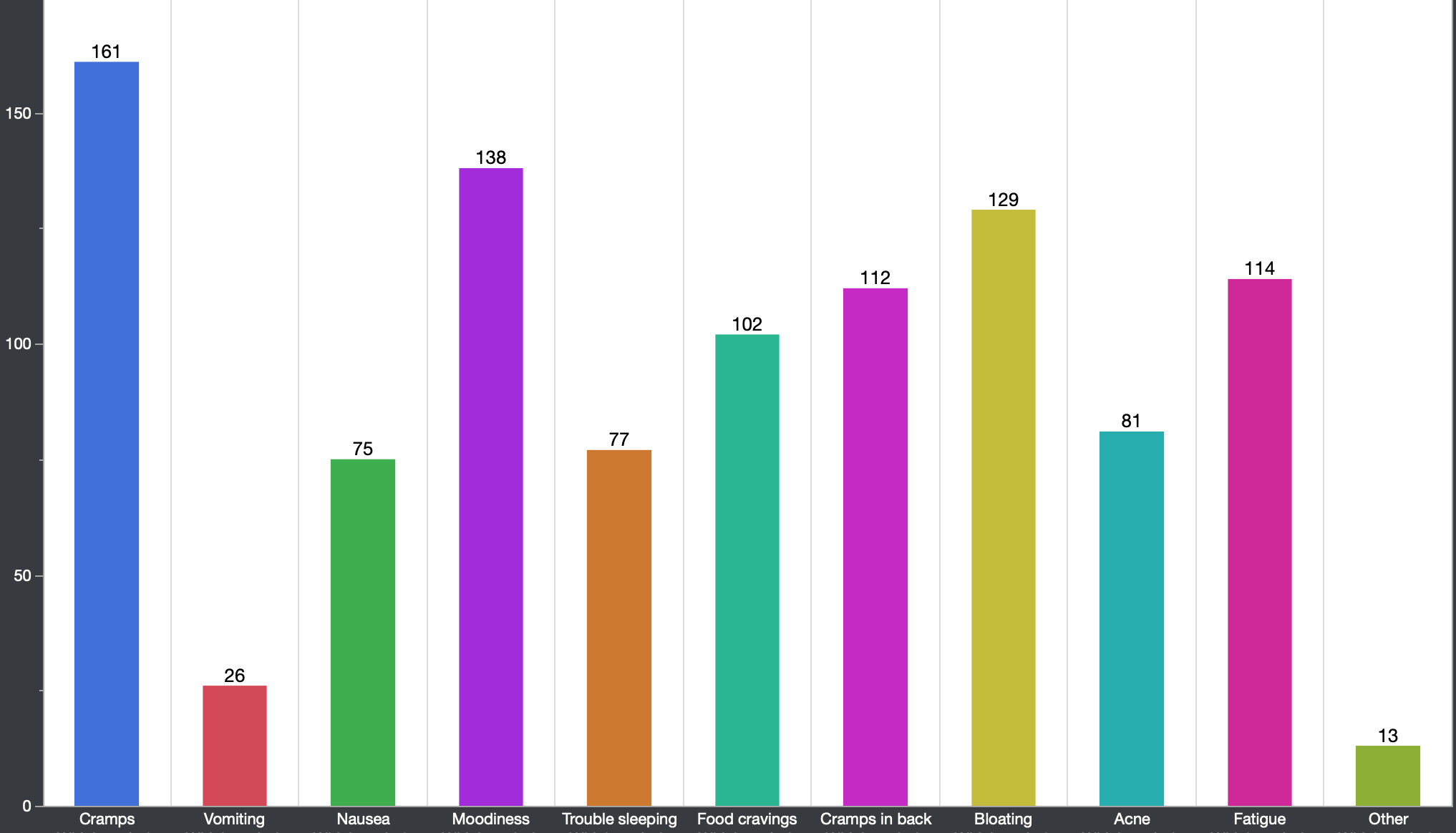
Which period symptoms do you experience (select all that apply)?
161 women in the cohort responded they experience cramps, 26 responded they experience vomiting, 75 responded they experience nausea, 138 responded they experience moodiness, 77 responded they experience trouble sleeping, 102 responded they experience food cravings, 112 responded they experience cramps in back, 129 responded they experience bloating, 81 responded they experience acne, 114 responded they experience, and 13 responded they experience other symptoms (Fig. 3).

Have you ever left school or work early because of cramps?
65.5% of the cohort answered yes and 35.5% said no.
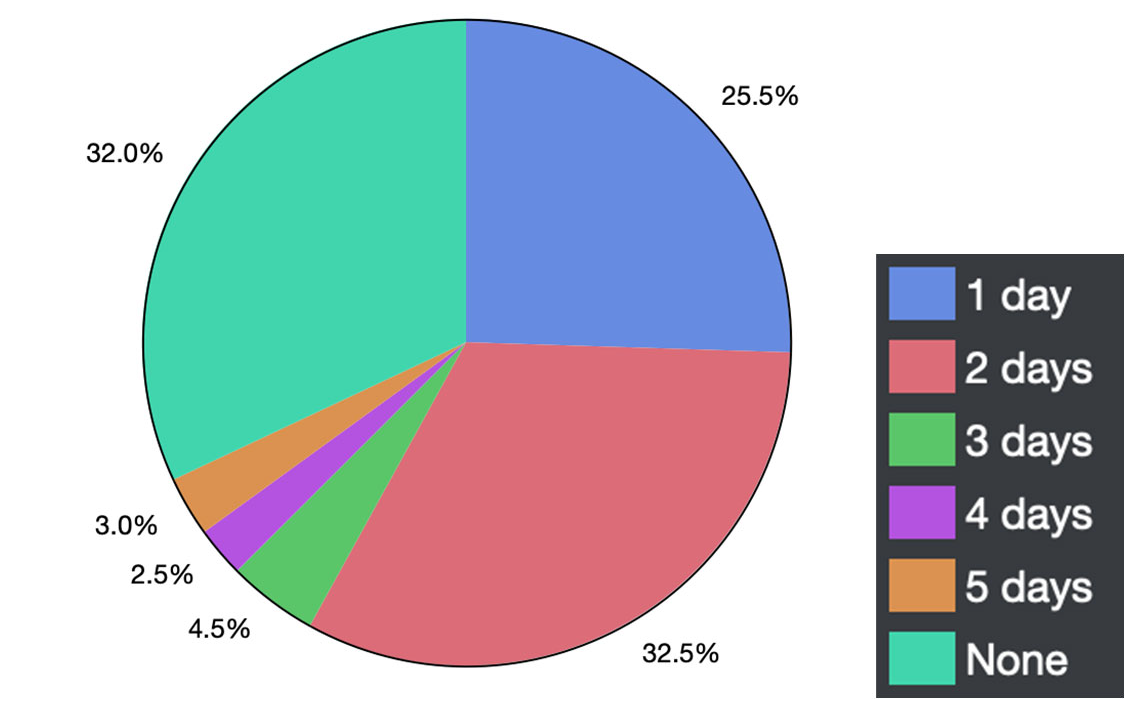
How many days at a time have you missed school or work because of your period?
25.5% of the cohort responded 1 day, 32.5% responded 2 days, 4.5% responded 3 days, 2.5% responded 4 days, 3.0% responded 5 days, and 32.0% responded zero days (Fig. 4).

Have you missed exams or standardized tests (AP exams, SAT, ACT, etc.) and had to reschedule them because of your period?
15% of the cohort answered yes, 49.5% said no, 35.5% responded with not in school.
Has staying home from school because of your period affected your grades?
17% answered yes, 47.5% said no, 35.5% responded with not in school.
Have you had to skip sports or a tournament/competition or other extracurricular activities because of your period?
35% answered yes, 29.5% said no, 35.5% responded with not in school.
Have you missed an opportunity for a promotion because of missing work due to your period?
19% answered yes, 63.5% said no, 17.5% answered with do not work.
Have you missed important work meetings because of your period?
22.5% answered yes, 58.5% said no, 19% answered with do not work.
Has your period prevented you from going out with friends?
68% of the cohort answered yes and 32% said no.
If you take medications for pain, which medications do you take (select all that apply)?
143 women in the cohort responded that they take ibuprofen, 51 responded that they take naproxen, 93 responded that they take acetaminophen, 26 responded that they take midodrine, 37 responded that they take aspirin, 10 responded that they take oxycodone, 17 responded that they take hydrocodone, 8 responded that they take other medications, and 11 responded that they take no medications (Fig. 5).

Are you prescribed birth control pills to help with menstrual cramps/heavy blood flow?
29.5% of the cohort answered yes and 70.5% said no.
What are some other things you do to help your period symptoms (select all that apply)?
34 women in the cohort responded that they have implemented a diet change, 58 responded that they exercise, 116 responded that they use heating pads, 124 responded that they sleep or rest, 103 responded that they drink more water, 44 responded that they manage their stress, 31 responded that they take baths, 11 responded they do other things to help with their symptoms, and 21 responded with none of the above (Fig. 6).

Contraceptive use by Income, Age, and Education
Question 13 of our survey asked whether participants have used oral contraceptive pills to assist with cramps and heavy blood flow. While race (p = 0.882) and marital status (p= 0.198) were not statistically significant for which participants are using OCPs, by contrast, income (p = 0.049), age (p = 0.002), and education (p = 0.002) were found to be significant predictors. Figure 7 displays the relationship between oral contraceptive use and income.

The plot above shows that over half of higher income groups actively use oral OCPs—53.3% of those from households that earn between $100,000 - $124,999 and 71.4% of those that earn $125,000 - $149,999 annually. Conversely, over 75% of participants in lower income groups do not regularly use birth control pills.
When grouping participants by education, individuals who were either currently enrolled in high school or whose highest level of education was completing high school were at significantly lower rates of taking an oral contraceptive (p = 0.028). On the other hand, individuals who have been enrolled in postgraduate studies were more likely to consume birth control medication (p = 0.007).
Discussion
Dysmenorrhea was highly common within our cohort at a rate that is similar to the estimated prevalence.1,2 In our study, 84% of participants reported moderate to severe pain (rated 3 and higher on a 1-5 scale) due to cramps. 87% of individuals described their menstrual flow as between medium and very heavy. This information supports that our cohort experienced symptoms of dysmenorrhea at high rates. The impact symptoms have on daily activities is variable. While 65.5% of our cohort reported having left work or school early due to painful cramps, 90% of this subpopulation was away from obligations for 2 days or less. However, these symptoms have had a considerable impact on social interactions and extracurricular activities. While 68% of people have chosen not to spend time with friends, 35% have skipped extracurricular events due to symptoms related to their period. These questions help clarify the extent to which dysmenorrhea is widespread and the quality-of-life implications associated with the condition.
Treatment for dysmenorrhea usually begins with pain relief medication and occasionally hormonal birth control or surgery in cases of underlying disorders. Non-steroidal anti-inflammatory (NSAID) drugs are most commonly used for pain including celecoxib, ibuprofen, mefenamic acid, and naproxen.2 While no specific NSAID has been proven particularly effective, a provider’s recommendation should be based on adherence and tolerability for the patient, based individually. These medications should be taken one to two days before menses and continued for up to three days following menses onset.
Oral contraceptives may be prescribed to reduce painful menses by helping decrease prostaglandin release and preventing ovulation. In a trial including 661 women, 63% initially suffered from dysmenorrhea. After 12 months of OCP use, 12% reported that the pain persisted.5 While there are mixed results, it is generally accepted that OCPs are likely to help.6,7 However, our study highlights an accessibility issue for OCPs. While the use of contraceptive pills is 40%, 71.4%, and 53.3% for the three highest income groups, respectively, the lowest income groups had usage rates of 20.4% and 23.2%. When NSAIDs are inadequate in the treatment for dysmenorrhea, it is possible that OCPs may not be available to patients who need them.
Access to OCPs may be influenced by income level. Cost as a barrier has been partly addressed by the Health and Human Services protocol from 2011 by requiring private insurance plans to cover the costs of contraceptive pills.8 However there is also the limitation of a prescription being required to obtain OCPs. Low-income female patients may have difficulty accessing their physician as needed to fill their prescriptions either due to transportation constraints or lack of general ease. 40% of low-income participants who were not using OCPs reported a willingness to take oral contraceptives if available in pharmacies without the need for a prescription. Moreover, 28% have reported troubles in accessing a prescription in general or when needed.9 When patients are in need of OCPs for contraceptive purposes or to assist with dysmenorrhea, it could be useful for clinicians to consider their overall access and resource levels.
Limitations
Survey research is vulnerable to reporting bias wherein participants feel compelled to answer according to a perceived “correctness” or in a way that exaggerates aspects of the disease state. In addition, using a third-party survey provider limits the population of respondents by sampling only people with incentives to complete surveys, thereby limiting the study’s external validity. Despite these shortcomings, the survey study provides valuable insight into the prevalence of dysmenorrhea and the underlying relationship between demographic factors and access to oral contraceptives.
Conclusion
Dysmenorrhea is widely common yet often goes unaddressed. Over 80% of this cohort has experienced moderate to severe pain and over one hundred participants have left work or school early as a result of cramps. Aside from professional obligations, dysmenorrhea takes a toll on social and extracurricular activities. While pain relief medication is considered as a first option to help with cramping, oral contraceptive pills may help prevent ovulation and decrease prostaglandin release. However, OCPs are not readily available to the general population, particularly women in low-income communities. Physicians should consider the background of their patient in the care of dysmenorrhea and explore affordable options to treat painful cramps as they can have a considerable impact on quality-of-life.
Ethics approval and consent to participate
This study was conducted in accordance with the Declaration of Helsinki. This study was given an exempt determination by our institutional review board # 2022-887.
Consent for publication
Not applicable, study given human subjects exempt determination
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests
The authors declare that there are no conflicts of interest.
Availability of data and material
Not applicable