1. Introduction
Patients with chronic illnesses experience various long-term adverse impacts on their physical, social, and psychological functioning.1 Chronic illnesses present continuous stressors that threaten many aspects of individual well-being, including the ability to fulfill personal, social, and professional roles and responsibilities.1 Chronically ill patients are confronted with a multitude of challenges, including physical pain, emotional coping, difficulties maintaining everyday skills and competencies, and loss of independence.1 Research has reinforced the role of psychological resilience; the ability to successfully manage and adapt to life’s adversities,2 as a buffer against negative outcomes in response to stressful life experiences.
Resilience is a multi-faceted concept that includes many components, such as optimism, self-esteem, internal locus of control, social connections, spirituality, and self-efficacy.3 While definitions of resilience vary widely, one of the main indicators of resilience is the ability to return to or maintain normal functioning after adverse life experiences. Research demonstrates that chronically ill patients with higher resilience levels display improved overall well-being. Among patients with chronic physical illnesses, studies have demonstrated that resilience is associated with self-care, improved life quality, adherence to treatment, physical activity, empowerment, self-efficiency, reduced mental health problems, and faster recovery.4
Similarly, a systematic review of studies on resilience within various types of physical illnesses ysshowed that psychological factors associated with resilience were self-esteem, internal locus of control, optimism, mastery, hardiness, hope, self-empowerment, acceptance of illness, determination, social support, and coping strategies including positive cognitive reappraisal, spirituality, active coping, and mastery.5 Moreover, a systematic review of resilience among patients with chronic physical diseases showed that resilience scores are higher among patients with more lethal diseases. Specifically, patients with cancer and cardiovascular diseases had higher resilience levels than patients with other diseases.4 The present study focuses on examining the role of psychological resilience in the social and professional functioning of patients with less severe chronic illnesses, namely diabetes, multiple sclerosis, and rheumtism.
Diabetes is one of the most prevalent chronic illnesses worldwide. More than 8% of adults had diabetes in 2014, and it was the direct cause of 1.5 million deaths in 2019.7 The premature mortality rate due to diabetes increased in both high-income and lower-middle-income countries over the past decade.6 Studies report prevalent rates of depression and anxiety among those living with diabetes. Specifically, depression is two to three times higher among individuals with diabetes while anxiety presents in approximately 40% of patients.7
In comparison to diabetes, the global prevalence of multiple sclerosis (MS) is very low (35.9 per 100,000 population.) However, prevalence rates of MS have also been rising worldwide since 2013.8 MS is an autoimmune disease that attacks the central nervous system and symptoms vary greatly and may include weakness in limbs, tremors, lack of coordination, vision problems, slurred speech, dizziness, and fatigue. Further complications that may develop include muscle stiffness or spasming, paralysis, difficulties in bladder, bowel, or sexual function, and mental health challenges. Some studies show that MS patients have a higher prevalence of emotional disorders relative to other patient groups with similar levels of physical disability.9 Specifically, research shows that 27 to 42% of MS patients experience depression.10 While 16 to 48% experience anxiety disorders.10 MS can often present during mid-life stages, and it can have unpredictable physical impacts, resulting in severe adjustment challenges.
Moreover, rheumatoid arthritis (RA) is one of the global leading causes of disability that affects approximately 1% of the world population. Similar to MS, RA is an autoimmune disease where the immune system attacks the tissue in body joints, causing joint swelling, pain, and stiffness. Left untreated, RA can lead to joint deformities and loss of joint functioning. Research shows that RA patients exhibit higher rates of depression and anxiety. Specifically, one study indicated that the total prevalence of anxiety, depression, and mixed anxiety-depressive disorder was found to be 70.8% among RA patients.11
2. Literature Review
As highlighted above, psychological resilience plays a role in moderating the impact of chronic illnesses on patient functioning. The literature indicates that this effect holds true for the three chronic illnesses presented above. Resilience variables that facilitate coping with stress have been linked to lower distress and lower glycosylated haemoglobin levels.12 A review that examined the impact of positive psychology on diabetes outcomes showed that positive personal characteristics such as self-efficacy, self-esteem, resilience, and adaptive coping are associated with better diabetes management and glycemic control across the lifespan.13 The review supports interventions that nurture personal resources among diabetes patients. Similarly, a study of 110 young adult participants with diabetes showed that self-esteem and self-efficacy positively predicted self-care behaviors and physiological outcomes13
Moreover, a longitudinal survey of 111 patients with diabetes tested glycosylated haemoglobin levels at baseline and 1-year follow-up.14 Results showed that individuals with higher resilience are less likely to have worsening glycosylated haemoglobin levels one year later. The study highlighted strong correlations between diabetes-related distress and increases in glycaemia among patients with low to moderate resilience scores but not among those with high resilience scores. In addition, the study indicated that patients with low resilience engaged in fewer self-care behaviors when they experienced increasing distress levels. Another study that included 60 patients with diabetes, hypertension, and rheumatoid arthritis showed that the hardiness characteristic, referring to the ability to endure difficult experiences, was significantly correlated with physiological adaptation only among patients with diabetes.15 Furthermore, a study of 50 elderly patients with diabetes indicated a significant correlation between hardiness and compliance to a prescribed diabetic regimen.15 As demonstrated by these studies, the positive impact of resilience variables on daily functioning among patients with diabetes is largely moderated by the facilitation of self-care and compliance behaviors that allow for illness control and management. This moderating factor is somewhat unique to diabetes, as treatment requires higher levels of self-management compared to other chronic illnesses.
Relative to diabetes, very few studies have examined the impact of psychological resilience on mitigating the negative effects of MS and RA on well-being. However, one study examined the role of benefit finding in predicting adjustment to MS over a 12-month interval.16 Benefit finding refers to the identification of benefits amid adversities.16 In the context of physical illness, benefit finding involves a re-evaluation of illness impacts in a more positive light. Pakenham and Cox’s study of 408 patients with MS showed that benefit finding factors, including compassion, spiritual growth, mindfulness, family relations growth, lifestyle gain, personal growth, and new opportunities accounted for more positive adjustment outcomes in relation to positive states of mind, positive affect, anxiety, and depression. Further, the study showed that benefit finding increases with time and tends to emerge later in the adjustment process. Follow up studies on benefit finding in MS patients highlighted similar results: enriched relationships, spiritual growth, family relations growth, lifestyle gains, inspiration, and relationship opportunities predicted positive affect and life satisfaction.17 A similar study among 364 patients with RA highlighted that benefit finding is positively correlated with more positive mental health, a larger social support network, and improved performance of self-care tasks.18
Moreover, one study explored the relationship between optimism and adaptation in a sample of 166 patients with MS or Parkinson’s disease.19 Results demonstrated that optimism had a positive impact on physical autonomy and emotion-oriented coping leading to better adjustment and lower emotional preoccupation, particularly among patients with MS. Another study that included patients with MS and RA showed that spirituality, focus on the future, and a commitment to successful living were correlated to better adaptation to the illness20 Further, an older study of 211 adults with MS, RA, and hypertension showed that the hardiness characteristic was significantly associated with psychological and physiologic adaptation, involvement in health promotion activities, and participation in patient education programs.21 A similar study of 122 RA patients showed that hardiness is positively associated with a strong and more satisfying social support system.22
Further, a study of 298 RA inpatients in China showed that resilience mediates the association between disease activity and mental health-related quality of life.22 The study showed that resilience was positively correlated with mental health-related quality of life, which is negatively correlated to disease activity. Health-related quality of life has also been negatively correlated with self-efficacy levels among RA patients.23 Another study of 104 RA patients highlighted the role of psychological well-being as a predictor of RA patients’ vulnerability to developing depression.24 A study of 81 older women with RA further showed that emotional regulation and emotional intensity predict emotional responses to painful symptoms.24 As explained earlier, emotional regulation is one of the main factors of psychological resilience. Similarly, research including 64 RA patients demonstrated that beliefs related to perceived control and self-efficacy significantly impacted degrees of adjustment and disability.25 Research also highlighted the role of resilience factors in predicting positive social interactions and next-week positive affect among a group of 82 RA and 88 osteoarthritis patients.25 A study of 154 RA patients showed that pain anxiety, pain and symptom self-efficacy, and coping strategies are significant predictors of functional status.26 Additionally, a study of 305 RA patients in China showed that perceived social support, hope, optimism, and resilience are negatively associated with RA-related fatigue.27 Optimism has also been negatively correlated with pain intensity and depressive symptoms among patients in the early to intermediate stages of RA.28 Overall, findings highlight the role of various resilience factors in mitigating the negative functional impacts of diabetes, MS, and RA.
Accordingly, The goal of the present study is to investigate the role of psychological resilience in the social and professional performance of patients with diabetes, MS, and RA. As demonstrated by past studies, psychological resilience impacts the trajectory of disability by playing a key role in buffering the negative impacts of chronic illnesses on psychological and physical health as well as daily functioning. However, the role of resilience in the trajectory of functional limitations among patients with diabetes, MS, and RA remains poorly researched.
3. Research statements
In this research the authors hypothesize that the social and professional performance of patients with higher levels of resilience will be less impacted by illness-related symptoms, while the performance of patients with lower levels of resilience will be more significantly impacted by illness-related symptoms among patients with diabetes, MS, and RA. Such investigation can provide healthcare providers with good guidelines to integrate mental health support into healthcare sittings. This study will answer the highlighted research questions " Does psychological resilience predict the performance of social and occupational functions in patients with diabetes, multiple sclerosis and rheumatoid arthritis?
4. Methodology
4.1. Sample characteristics
A total of 301 convienience individuals (58.8% female) participated in the present study, as shown in Table 1. More than three quarters of participants (77.41%) were married. Further, more than a quarter of participants were 50-59 years old (27.76%). Around 23% were 40-49 years old, 17.39% were 30-39 years old, 16.05% were over 60 years old, and around 15% were 20-29 years old. Nearly half the sample were housewives (47.51%). Around 20% were employed, nearly 19% were unemployed, around 4 % were students, and around 7% were retired. In addition, approximately 44% of participants are diagnosed with diabetes, while 28% are diagnosed with rheumatoid and around 25% are diagnosed with MS. The majority of participants have had the diagnosed illness for more than three years (72.39%).
4.2. Study instruments
Two psychometric measures were used to achieve the objectives of the present study: the Psychological Resilience Scale and the Performance of Social and Occupational Functions Scale.
4.2.1. The Psychological Resilience Scale
The Psychological Resilience Scale originaly was developed by Connor and Davidson.29 Consists of 25 items that evaluate participants’ level of psychological resilience and ability to manage challenges. Items are scored on a 5-point scale ranging from ‘Strongly Agree’ (5 points) and ‘Strongly Disagree’ (1 point). Thus, the overall score ranges from 25 to 125 points, where a higher score indicates a higher degree of psychological resilience. In order to ascertain the reliability of the scale, the Alpha Cronbach formula was used to calculate the internal consistency of the scale, which was 0.94. This factor indicates an appropriate level of reliability for the purposes of the present study. All items were also correlated to the overall score at a value higher than 0.30, indicating that the scale has a high degree of internal validity.
4.2.2. The Performance of Social and Occupational Functions Scale
The social and occupational functions scale SOFSE originally was developed by Wang, et al.29 The final scale had 30 items in six dimensions. The scale showed that internal consistency coefficients and test–retest reliabilities for each dimension ranged from 0.70 to 0.84 and 0.72 to 0.89, respectively. Moreover, criterion-related validity was demonstrated by the significant correlations between the SOFSE and the following measures: the Mini Mental Status Examination (r = 0.60, p < 0.001), the Quality of Life in Epilepsy-31 (r = 0.53, p < 0.001).
In the current study, The social and occupational functions scale SOFSE consists from six subscales: relationships consists of 4 items, communication consists of 4 items, social activities consists of 5 items, entertainment activities consist from 2 items, life skills consists of 5 items and job functions consists of 10 items. All the the scale items is rated on a 4-point scale ranging from 0 to 3 representing participants’ evaluation on each items. The internal consistency Alpha Cronbach was calculated and it was (0.60. 0.75, 0.71, 0.50, 0.72, 0.72) for (relationships, communication, social activities, entertainment activities, life skills and job functions) respectively. All Alpha values are acceptable. In term of validity, all items were correlated to the overall score at a value higher than 0.30, indicating that the scales have a satisfactory degree of internal validity.
Also, a number of demographic information well collected about the study participant (gender, marital status, age, job status, Health status and Duration of illness).
4.3. Study procedures
Aligned with the Helsinki Declaration, ethical approval IRB for the current study was obtained from the ministry of health ethical research committee (Number:10696). Participants were informed of the objectives of the study and informed written consent was obtained from them. They were free to withdraw from the study at any stage; their information was kept confidential and used for research purposes only.
4.4. Data analysis
Data were entered and analyzed using the Statistical Package for the Social Sciences (SPSS), Version 25.0. Categorical variables were presented as frequencies and percentages and continuous variables as means and standard deviations. Also, simple regression, t-test and one-way ANOAV were used to analyse the study data and answer the study questions.
5. Results
Several statistical analyses were employed to answer study questions. Results are presented in this section.
5.1. Descriptive statistics
From the table (1) the performance of social and occupational function subscale among Diabetes, Multiple Sclerosis and Rheumatoid patients means ranges (1.62- 2.46), the highest means is for relationship subscales while the lowest means is for Job function/ unemployed. Also, the psychological resilience mean is 3.80. This result shows that performance of social and occupational function subscales levels is from moderate to high while the psychological resilience is at a high level.
5.2. Psychological resilience prediction on functioning was also studied. Different levels od prediction values were aotained among study variables as presented in table (2)
The result in table (2) shows that the prediction of the psychological resilience in performance of social and occupational functions for(relationship) subscale (R = 0.51, F= 24.98, p ≤ 0.05) among MS patients. This result means the psychological resilience positively predict the relationship and explained (26%) of the variance. Also, table (2) result shows that the psychological resilience in performance of social and occupational functions for(relationship) subscale (R = 0.34, F= 17.13, p ≤ 0.05) among Diabetes patients. This result refers to the psychological resilience positively predicting the relationship and explaining (12%) of the variance. While the result of the psychological resilience in performance of social and occupational functions for(relationship) subscale (R = 0.17, F= 2.56, p ≥ 0.05) among Rheumatoid patients. This result means that psychological resilience doesn’t predict the relationship. This result shows that psychological resilience in the performance of social and occupational functions for(relationship) is better predicted among MS patients.
Also, the prediction of the psychological resilience in performance of social and occupational functions for (communication) subscale (R = 0.49, F= 22.11, p ≤ 0.05) among MS patients. This result means the psychological resilience positively predict the communication and explained (23%) of the variance. Also, table (2) result shows that the psychological resilience in performance of social and occupational functions for (communication) subscale (R = 0.33, F= 16.59, p ≤ 0.05) among Diabetes patients. This result refers to the psychological resilience positively predicting the communication and explaining (10%) of the variance. While the result of the psychological resilience in performance of social and occupational functions for (communication) subscale (R = 0.23, F= 4.52, p ≤ 0.05) among Rheumatoid patients. This result means that psychological resilience predicts the communication and explained (4%) of the variance. This result shows that psychological resilience in the performance of social and occupational functions for (communication) is better predicted among MS patients.
In addition to, the prediction of the psychological resilience in performance of social and occupational functions for (social activities) subscale (R = 0.43, F= 16.22, p ≤ 0.05) among MS patients. This result means the psychological resilience positively predict the social activities and explained (17%) of the variance. Also, table (2) result shows that the psychological resilience in performance of social and occupational functions for (social activities) subscale (R = 0.44, F= 30.86, p ≤ 0.05) among Diabetes patients. This result refers to the psychological resilience positively predicting the social activities and explaining (18%) of the variance. While the result of the psychological resilience in performance of social and occupational functions for (social activities) subscale (R = 0.20, F= 3.46, p ≥ 0.05) among Rheumatoid patients. This result means that psychological resilience doesn’t predict the social activities. This result shows that psychological resilience in the performance of social and occupational functions for (social activities) is better predicted among MS and diabetes patients nearly similar.
The prediction of the psychological resilience in performance of social and occupational functions for (entertainment activities) subscale (R = 0.30, F= 7>15, p ≤ 0.05) among MS patients. This result means the psychological resilience positively predict the entertainment activities and explained (9%) of the variance. Also, table (2) result shows that the psychological resilience in performance of social and occupational functions for (entertainment activities) subscale (R = 0.36, F= 19.05, p ≤ 0.05) among Diabetes patients. This result refers to the psychological resilience positively predicting the entertainment activities and explaining (13%) of the variance. While the result of the psychological resilience in performance of social and occupational functions for (entertainment activities) subscale (R = 0.36, F= 12.44, p ≤ 0.05) among Rheumatoid patients. This result means that psychological resilience predicts the entertainment activities and explained (13%) of the variance. This result shows that psychological resilience in the performance of social and occupational functions for (entertainment activities) is better predicted among Diabetes and Rheumatoid patients.
For the results of prediction of the psychological resilience in performance of social and occupational functions for (life skills) subscale were (R = 0.59, F= 37.91, p ≤ 0.05) among MS patients. This result means the psychological resilience positively predict the life skills and explained (35%) of the variance. Also, table (2) result shows that the psychological resilience in performance of social and occupational functions for (life skills) subscale (R = 0.25, F= 8.63, p ≤ 0.05) among Diabetes patients. This result refers to the psychological resilience positively predicting the life skills and explaining (6%) of the variance. While the result of the psychological resilience in performance of social and occupational functions for (life skills) subscale (R = 0.36, F= 12.12, p ≤ 0.05) among Rheumatoid patients. This result means that psychological resilience predicts the life skills and explained (13%) of the variance. This result shows that psychological resilience in the performance of social and occupational functions for (life skills) is better predicted among MS patients.
As shown in table (2), the prediction of the psychological resilience in performance of social and occupational functions for (work and job – employed) subscale (R = 0.32, F= 1.71, p ≥0.05) among MS patients. This result means the psychological resilience does not predict the work and job – employed. Also, table (2) result shows that the psychological resilience in performance of social and occupational functions for (work and job – employed) subscale (R = 0.63, F= 16.71, p ≤ 0.05) among Diabetes patients. This result refers to the psychological resilience positively predicting the work and job – employed and explaining (39%) of the variance. While the result of the psychological resilience in performance of social and occupational functions for (work and job – employed) subscale (R = 0.48, F= 3.87, p ≥ 0.05) among Rheumatoid patients. This result means that psychological resilience does not predict the work and job – employed and. This result shows that psychological resilience in the performance of social and occupational functions for (work and job – employed) is better predicted among Diabetes patients.
Furthermore, the prediction of the psychological resilience in performance of social and occupational functions for (work and job – unemployed) subscale (R = 0.52, F= 19.49, p ≤ 0.05) among MS patients. This result means the psychological resilience positively predict the work and job – unemployed and explained (27%) of the variance. Also, table (2) result shows that the psychological resilience in performance of social and occupational functions for (work and job – unemployed) subscale (R = 0.48, F= 28.71, p ≤ 0.05) among Diabetes patients. This result refers to the psychological resilience positively predicting the work and job – unemployed and explaining (23%) of the variance. While the result of the psychological resilience in performance of social and occupational functions for (work and job – unemployed) subscale (R = 0.39, F= 11.96, p ≤ 0.05) among Rheumatoid patients. This result means that psychological resilience predicts the work and job – unemployed and explained (15%) of the variance. This result shows that psychological resilience in the performance of social and occupational functions for (work and job – unemployed) is better predicted among MS and Diabetes patients.
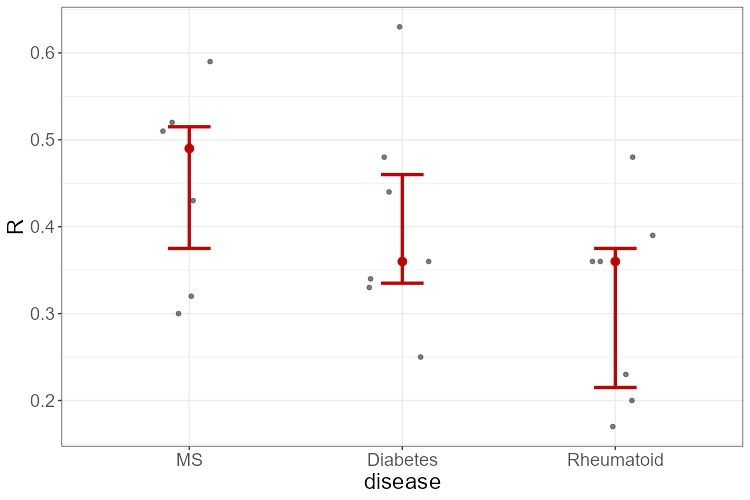
In summery, Graph (1) shows That MS population demonstrates high levels of resilience, as indicated by strong and consistent predictor values. In contrast, the Rheumatoid population shows weaker and less stable resilience predictors. This highlights the importance of considering resilience when designing interventions for individuals with MS conditions.

6. Discussion
The main purpose of the present study was to examine the role of psychological resilience in the social and professional performance of patients with chronic illnesses; specifically, MS, diabetes, and RA. Earlier studies have shown that higher levels of psychological resilience lead to improved well-being and psychological outcomes among chronically ill adults.30 The results of the current study are mostly in alignment with previous findings. Results revealed that psychological resilience was a positive predictor of various social and professional functions among all patients. Resilience best predicted social and professional functions among MS patients followed by diabetes patients and RA patients.
Specifically, psychological resilience positively predicted most aspects of social and professional performance among participants with MS, including relationships, communication, social activities, entertainment activities, life skills, and unemployment job functions. Studies on MS patients showed that benefit finding resulted in improved adjustment outcomes over a 12-month interval, including relationships, spiritual growth, lifestyle gains, and positive affect.18,31 Further, resilience positively predicted all aspects of social and professional performance among patients with diabetes, including relationships, communication, social activities, entertainment activities, life skills, employment job functioning, and unemployment job functioning. As highlighted by previous findings, resilience variables such as self-efficacy, self-esteem, and adaptive coping are correlated with improved diabetes management and glycemic control.13 Research shows that higher resilience is also associated with lower declines in glycosylated haemoglobin levels over the span of one year.14 Therefore, resilience is correlated with better performance outcomes among patients.
Psychological resilience was also a positive predictor of social and professional performance among RA patients only in terms of communication, entertainment activities, life skills, and unemployment job functioning. In alignment with these findings, previous studies highlight the benefits of resilience variables such as benefit finding with improved mental health, social support, and self-care.18 Other studies show that resilience mediates the relationship between RA disease activity and mental health-related quality of life in nearly 300 patients in China.23 Overall, psychological resilience accounted for the least variance in the social and professional functioning of RA patients. This could be attributed to findings that indicate that RA is one of the most physically debilitating chronic illnesses in the world.30 The severity of physical disablement among RA patients relative to patients with MS or diabetes could limit the apparent impacts of psychological resilience on daily functions.
The effect of resilience was greatest for employment job functioning among diabetes patients, explaining 39% of the variance, while resilience did not predict employment job functioning among patients with MS and RA. This could be attributed to more adverse physical symptoms that result in lower work ability and higher unemployment rates in MS and RA patients compared to patients with diabetes.32 On the other hand, the effect of resilience was greatest for life skills functioning among MS patients, explaining 35% of the variance, while it only accounted for 6% of the variance among diabetes patients. This could also be explained by findings that indicate diabetes has a lower level of physical impairments and negative impact on personal independence compared to MS and RA.30
7. Conclusion
The results of the present study highlighted the positive impacts of psychological resilience on the social and professional functioning of patients with MS, RA, and diabetes. These impacts are most apparent and significant among patients with MS and diabetes. The findings indicate that interventions that improve levels of psychological resilience among patients with chronic illnesses could mitigate the negative effects of illness-related symptoms on social and professional functions. Further research is required to examine the causes of the differential impacts of resilience that were highlighted in this study on patients with varying chronic illnesses as well as on different aspects of social and professional performance. The positive role of employment in the maintenance and support of psychological resilience among chronically ill patients could also be further examined to inform potential interventions.
Acknowledgment
The authors thank all patients who participated in this study. Authors also appreciates the contribution of hospitals, medical centers ant the Jordanian Ministry of Health (MoH) how made data collection possible.
Disclosure statement
No potential conflict of interest was reported by the authors.
Data availability statement
Due to the patients’ privacy considerations, data will be available upon request to the corresponding author.
Author contributions
AA was responsible for creating the manuscript idea, the data collection and entry, drafting the manuscript, designing the study. AQ was responsible for data analysis and interpreted the results. All authors reviewed the final manuscript and provided their consent.