Introduction
There are many factors that contribute to healthcare seeking behaviors. In various studies, three main themes have shown up: apprehension about antenatal, prenatal, and postpartum care services, disruptions in provider care or location, and changes in social support. In terms of apprehension about care, women were often concerned about inadequate provision of resources to support emotional and mental well-being.1 Disruptions in provider care and social support were related to delayed care, poor communication, and a lack of the women’s involvement in decision making.2 These significantly affected OB/GYN care seeking behavior and willingness to give birth at healthcare facilities.
Stigmas are powerful social processes that are characterized by labeling, stereotyping, and separation, leading to status loss and discrimination, all occurring in the context of power.3 Healthcare related stigma negatively affects people seeking help at a time when they need it most. Stigma within health facilities can manifest in a variety of ways, such as denial of care, providing mediocre care, physical and verbal abuse, and/or making people feel unheard or unattended to.3 This can result in people not wanting to seek care regardless of how necessary it may be. Stigma is another factor that contributes to one’s willingness to seek care, and in this case, a woman’s willingness to seek professional OB/GYN care.
Several survey studies have attempted to understand the different factors that encourage and discourage OB/GYN care seeking behaviors in women. A study of women in Madagascar aimed to identify and analyze the factors that influence the utilization of maternal services.2 The researchers found that among the 245 women surveyed, 13.9% did not attend any antenatal care (ANC) visits. School level and occupation positively influenced the likelihood of attending ANC visits. A lack of preparation, including financial and logistics problems, and the women’s low involvement in decision making at delivery were barriers to willingness to give birth at healthcare facilities. Similarly, a study of women in the Wa Municipality of Ghana focused on assessing how women felt about the quality of their maternal healthcare and what factors contributed to high quality maternal healthcare.4 The researchers found that logistics and equipment, lack of empathetic service delivery, inadequacy of care providers, and affordability of service affected the women’s satisfaction and seeking of care.
These studies focused on minoritized women in developing countries, but a comparative study between women in Ghana and women in the United States was also conducted. In this study, many similarities were found between the groups of women regardless of their different economic and cultural background. Both Ghananian women and American women reported that they felt apprehensive about the care that they were receiving and were often not given the option to have in-person appointments because of the pandemic. Although American women reported less access to care issues, both groups felt that their healthcare providers couldn’t address the impact of their pregnancies on their mental health. In both countries, pregnant women reported that they were left to make critical healthcare decisions on their own, filling in gaps in their care using the knowledge they had gained from previous pregnancies and prior healthcare experiences.1 The overall lack of support and clarity left many of these women unwilling to routinely schedule and show up at their appointments.
There are many variables that can further contribute to OB/GYN healthcare seeking behavior amongst women. We aimed to investigate the health status and experiences of women ages 16-80 to determine whether we can use these experiences to predict which women will seek routine OB/GYN checkups and care
Methods
The survey
Two hundred women were surveyed through a survey research platform. The survey consisted of 13 questions designed to assess factors that affect whether or not women will seek OB/GYN care. Questions 1, 2, 4, and 5 were adapted from the NIH Healthcare Access and Utilization Survey.5 For some of the questions, multiple selections amongst the multiple choices were allowed, so the percentage totals could exceed 100%. The first two questions inquired about the last time that the women had visited a health professional and/or OB/GYN. The third question asked about whether the participants had any chronic health conditions. The 4th and 5th questions assessed whether or not the participants felt respected by their healthcare providers. The rest of the questions focused on the care received during pregnancy if applicable.
Statistical analysis
Data was analyzed using JMP Pro 16.2 for Windows. Variables were compared to one another to quantify cause and effect, and the fit modes used held all other variables constant to ensure that there were no confounding variables or other explanations for data trends. For comparing 2x2 contingency tables, Fisher’s two-tailed exact test was used. All results used weighting generated by the survey platform to match the univariate distributions of age and gender.
Ethical considerations
The study was exempt by the HCA Centralized Algorithms for Research Rules on IRB Exemptions (CARRIE)/ IRB manager, study number 2022-734.
Results
A total of 200 women were surveyed. The median age of the respondents was 38.5, the interquartile range of age was from 29-50 years, with a range of 16-77 years. 63% of the respondents were white, 17% were black, 9.5% were Hispanic, 4% were Asian, 1% were Latino, 1.5% were multiracial, 3% were of other races, and 1% preferred not to say. The composition of race in this survey population roughly approximates that of the United States. Race was elected by the survey participant.
2% of the respondents have completed middle school, 42% have completed high school, 23.5% have completed an undergraduate degree, 20.5% have completed vocational/technical training, and 12% have completed a postgraduate degree. 26% were in low income level 1, 32% were in low income level 2, 10% were in middle income level 1, 12.5% were in middle income level 2, 6% were in high income level 1, 4% were in high income level 2, 3.5% were in high income level 3, and 6% preferred not to say. Low income level 1 is defined as people who make under $25,000. Low income level 2 was defined as people who make between $25,000 and $49,999. Middle income level 1 was defined as people who make between $50,000 and $74,999. Middle income level 2 was defined as people who make between $75,000 and $99,999. High income level 1 was defined as people who make between $100,000 and $124,999. High income level 2 was defined as people who make between $125,000 and $149,999. High income level 3 was defined as people who make between $150,000 or more. Each question in the survey will be explored in this section.
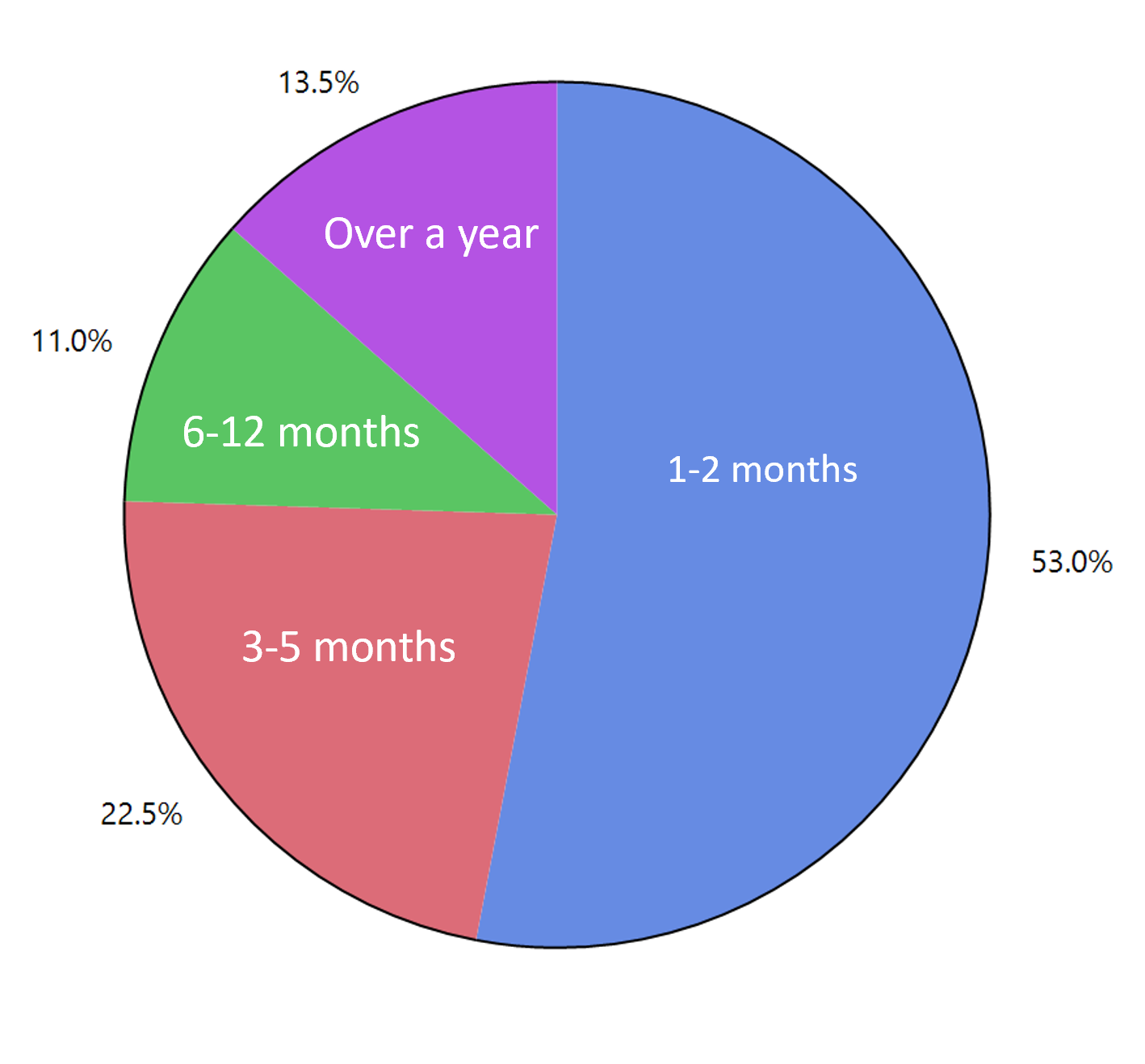
How long has it been since you last saw a doctor or other health care professional?
53% of women responded that they had seen a doctor or healthcare professional within the last 1-2 months. 22.5% responded that they had seen a doctor or healthcare professional within the last 3-5 months. 11% responded that they had seen a doctor or healthcare professional within the last 6-12 months, and 13.5% responded that it had been over a year since they had seen a doctor or a healthcare professional. The results are summarized in Figure 1 below.

In the past year, have you seen a doctor who specializes in women’s health (an obstetrician/gynecologist)?
60% of women responded yes and 40% responded no.
Have you been diagnosed with any chronic health conditions?
Respondents could pick multiple options for this question. 45% of the women responded that they had some mental health disorder. 17% responded that they had obesity. 7% responded that they had diabetes. 10.5% responded that they had hypertension. 2% responded that they had heart disease, 1% responded that they had liver disease, and 1% responded that they had kidney/renal disease. 16.5% responded that they had anemia.
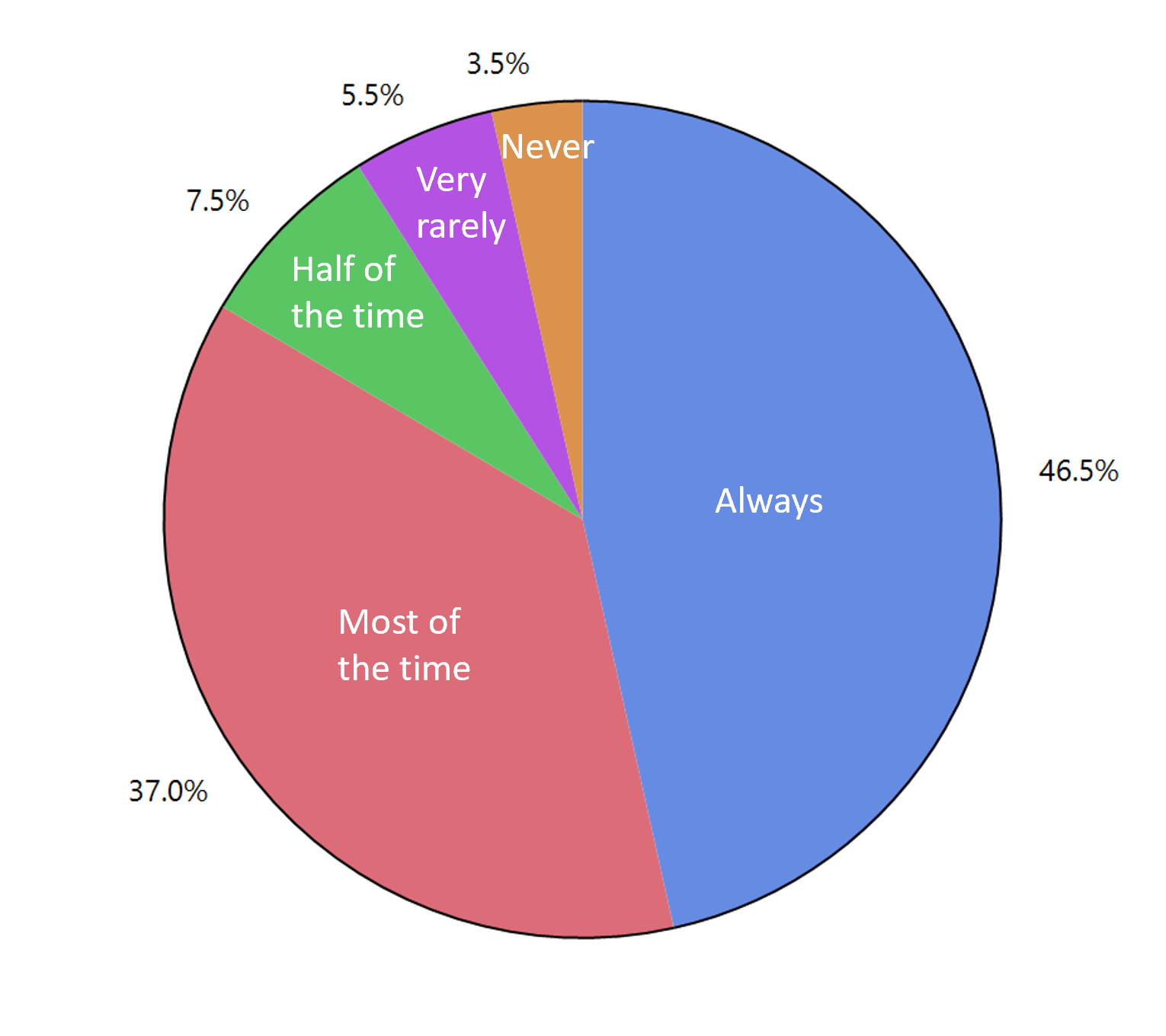
How often were you treated with respect by your doctors or health care providers?
46.5% of women responded that they were always treated with respect by health care providers. 37% responded that they were treated with respect most of the time. 7.5% responded that they were treated with respect half of the time. 5.5% responded that they were treated with respect very rarely. 3.5% responded that they were never treated with respect. The results are summarized in Figure 2 below.

How often did your doctors or health care providers ask for your opinions about your medical care? For example, what kind of tests, procedures, or medications you prefer.
22% of the women responded “Always”. 35.5% responded “Most of the time”. 21% responded “Half of the time”. 13% responded “Very rarely”. 8.5% responded “Never”. It should be noted that the women who felt that they were asked for their opinions about their medical care were also significantly more likely to feel respected by their healthcare providers (P <0.0001).
Were you seeing an obstetrician/gynecologist during your pregnancy(ies)?
66% of the women who responded had been pregnant. 82.58% were seeing an OB/GYN for their entire pregnancy(ies). 8.33% responded that they were seeing one for most of their pregnancy(ies). 2.27% responded that they were seeing one for half of their pregnancy(ies). 2.27% responded that they were seeing one at the end of their pregnancy(ies). 4.55% responded that they had never seen an OB-GYN.
Throughout your pregnancy(ies), where did you learn about how to have a healthy pregnancy?
For this question, respondents could pick multiple options. 46.64% of the women responded that they got their information from an obstetrician/gynecologist. 15.13% responded that they used the internet. 22.27% responded that they got information from friends and family. 13.03% responded that they learned from previous pregnancies, and 2.94% responded “None of the above”. It is interesting to note that over half of the women received their information from sources other than a professional medical practitioner.
During and after your pregnancy, who did you have physical support from?
For this question, respondents could pick multiple options. 33.87% of the women said they had support from their obstetrician/gynecologist. 25% responded that they had support from friends. 37.5% said they had support from family. 3.63% said they didn’t have any physical support.
During and after your pregnancy, who did you have emotional support from?
For this question, respondents could pick multiple options. 22.65% of the women responded that they had support from their obstetrician/gynecologist. 29.06% said they had support from friends. 44.44% said they had support from family, and 3.85% said they didn’t have any emotional support. Note that OB/GYN specialists provided support for a very small portion of women.
A multivariate analysis was done to look for associations between whether respondents had seen an OB-GYN in the past year. Factors that were positively correlated included older age (P=0.0259), white race (P=0.0323), and those who were asked more often for their opinions about their healthcare (P=0.0002). This last point is perhaps the most important result of the study. Patients’ personal experience with their doctor dictates future healthcare seeking behavior. When women feel heard and respected, they are more likely to continue seeing their doctor.
Discussion
Several factors, such as stigma, bias, and lack of knowledge about care can affect women’s willingness to seek out OB/GYN care. Consistent with our survey results, several other studies have found three main themes that affect willingness to seek OB/GYN care: apprehension about care services, disruptions in provider care or location, and changes in social support.1 Logistics and equipment, lack of empathetic service delivery, inadequacy of care providers, and affordability of service affected the women’s satisfaction and seeking of care.4 Additionally, women in both developing and developed countries reported that they felt apprehensive about the care that they were receiving and were often not given the option to have in-person appointments. They also felt that their healthcare providers couldn’t address the impact of their pregnancies on their mental health and were left to make critical healthcare decisions on their own, filling in gaps in their care using the knowledge they had gained from prior healthcare experiences.1 The overall lack of support and clarity left many of these women unwilling to routinely schedule and show up at their appointments.
Our survey results concur with these reports. Almost half of the women that we surveyed have not visited an OB/GYN in the past year, and nearly all of them reported that they did not feel respected by their healthcare providers and weren’t asked for their opinions about their healthcare. The feeling of not being respected or heard by healthcare providers could be due to racial/socioeconomic bias, patient’s limited knowledge of their options, and lack of physical/emotional support and understanding. Our survey found that Black and Hispanic women felt disrespected and/or unheard by their healthcare providers more often than white women. This finding may contribute to the worsening disparities in reproductive health outcomes between these groups of women. In particular, not having regular OB/GYN appointments puts women at higher risk for adverse reproductive health outcomes, such as having undiagnosed cancer or STDs, and at higher risk for having unplanned, unsupported, and/or high risk pregnancies.6
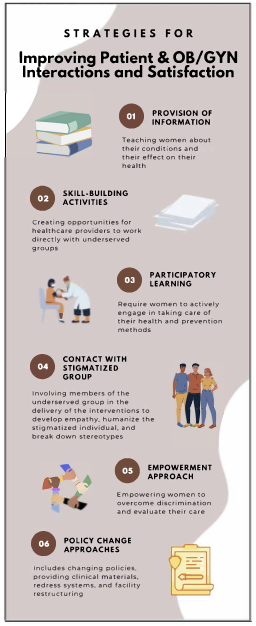
In addition to identifying various factors that affect healthcare seeking behaviors, several studies have explored what can be done to help mitigate feelings of being disrespected, unheard, or unsupported by healthcare providers. Several key strategies are detailed in figure 3.3,5

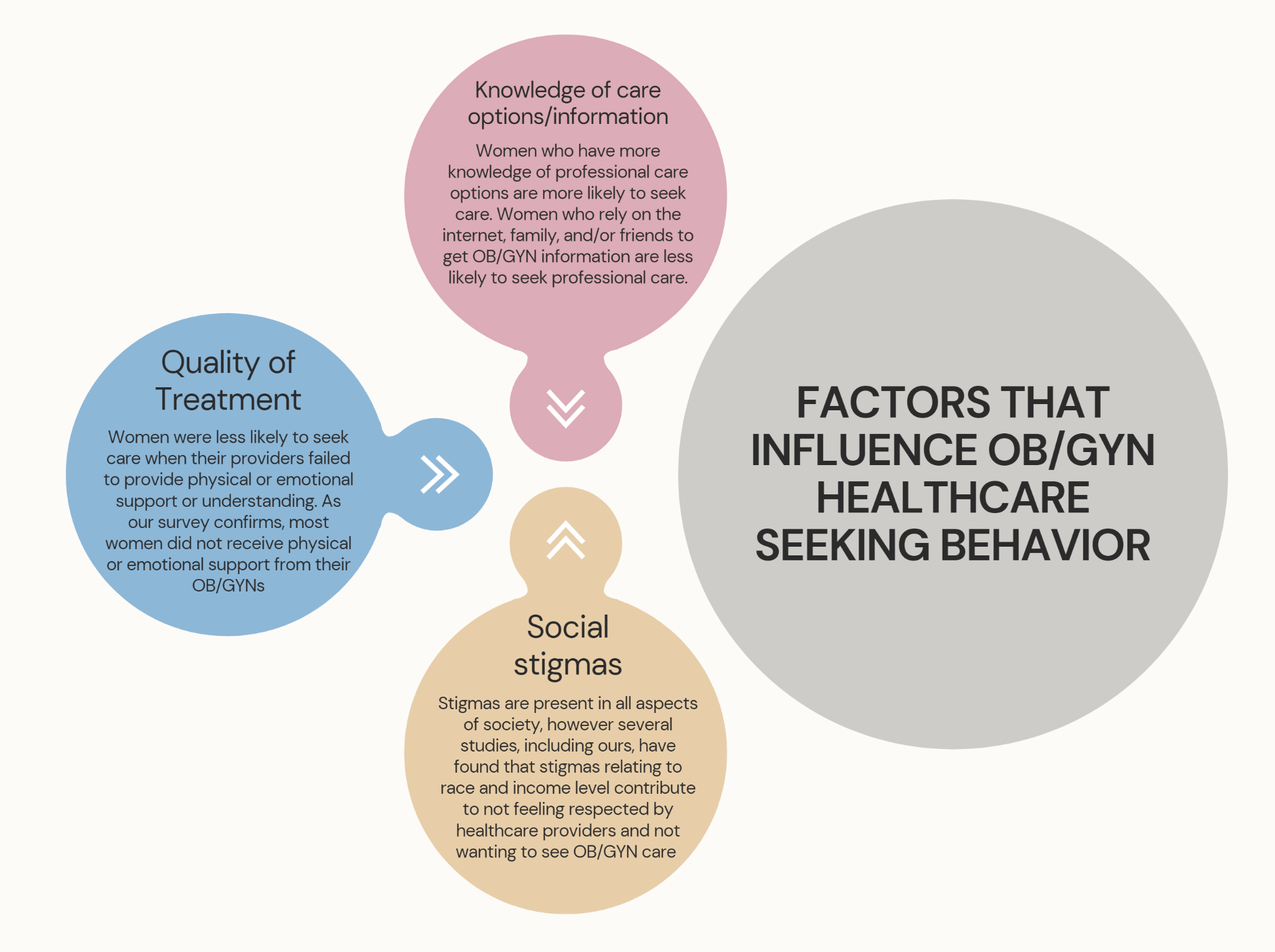
Over the past decade, increasing global access to maternal and OB/GYN healthcare has allowed for a united effort to decrease adverse reproductive and sexual health outcomes. However, disparities amongst different populations are still present despite these efforts. In particular, reproductive and maternal health disparities continue to be a large issue amongst non-white women. There are many factors that contribute to these trends, but one of the main ones is not having adequate professional OB/GYN care. For this, women are required to actively seek and receive care, but many report that they do not do so because they do not feel respected or heard by their healthcare providers. The factors that contribute to OB/GYN healthcare seeking behavior are summarized in figure 4.

Limitations
The survey results are limited because only women who were registered with our survey platform had the opportunity to participate in this survey. Additionally, only women in the United States were surveyed. Future studies could focus on getting detailed accounts of specific experiences of each woman and looking into other factors, such as location, preexisting health conditions, and family background. Additionally, a survey study could be done of OB/GYN healthcare providers and their experiences with patient care in various areas of the country. This way, the results of both studies could be compared to help identify gaps or areas of miscommunication between patient and provider, which could further improve positive healthcare experiences and outcomes.
Conclusion
It is important to recognize that in order to combat health disparities, efforts must be made to improve patient and provider interactions and satisfaction. In the future, healthcare should be focusing on ensuring that patients feel supported and understood, for this is the only way that we can make progress towards a healthier society.
Disclaimer
This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.