Introduction
Although urological practice guidelines recommend that physicians offer chaperones during sensitive exams, the consistent use of chaperones in clinical urological practice has not been previously studied.1 The demographics of urological patients differ from patients within obstetrics and gynecology, a field where chaperones are routinely utilized in practice. This, and other factors may be linked to differences in chaperone utilization within urology compared to other fields.2,3 Investigating these distinctions is essential to understanding the roles of chaperones in urology practice.
The purpose of chaperones in a clinical setting is to make a patient feel safe and respected and to provide protection for both the clinician and patient. The present investigation reviewed and attempted to synthesize patient and physician perspectives on chaperones; and identified barriers for operationalizing chaperones in urology practices.
Methods
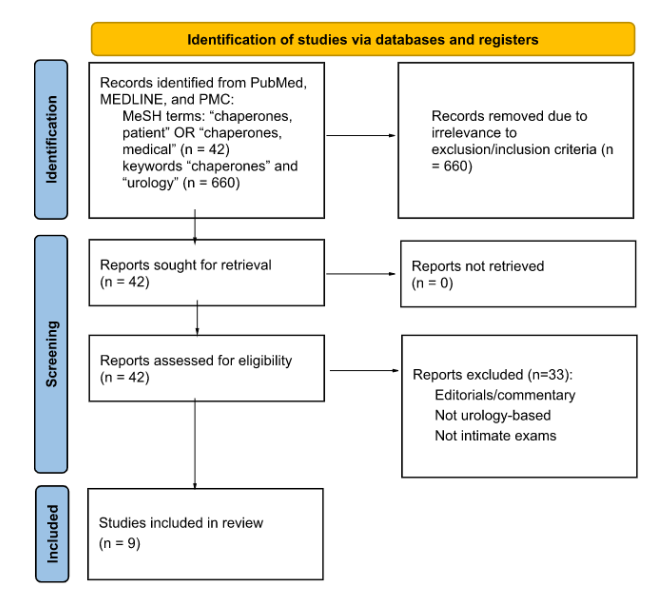
The PRISMA 2020 guidelines for systematic review methodology were referred to when appropriate for this review. Related to the small number of applicable studies, meta-analyses were not conducted. This review includes prospective, case-control, and retrospective studies that examined either patient or provider perspectives on the use of chaperones during urological exams. Studies that did not investigate either patient or provider perspectives for urological exams specifically, (i.e., studies in primary care or obstetrics and gynecology) were excluded. Searches were conducted in PubMed, MEDLINE, and PMC and used the following search protocol for all databases: 1) the MeSH terms: “chaperones, patient” OR “chaperones, medical” and 2) the keywords “chaperones” and “urology” to identify potential studies. Related to the limited number or articles included it is difficult to label this review as systematic.

Perspectives on Chaperones
Studies investigating patient perspectives on sensitive exams in primary care and obstetrics/gynecology demonstrate that patients generally do not wish to have a chaperone present for their examination.4–6 This holds true for sensitive exams within urology, 11.5-42% prefer chaperones, (Table 1) and is especially pronounced for male patients, who prefer the presence of a chaperone less than female patients.4,7,8 Patients reported trust in their provider, and lack of comfort or embarrassment with sensitive exams as reasons for not wanting a chaperone present.4
Patient preference around chaperone use during urologic examinations, however, is more nuanced. In an earlier study, the majority (73%) of male urology patients felt a chaperone should be offered for every encounter while a smaller group (14%) actually prefer a chaperone to be present.9 A later study confirmed this finding, revealing that the vast majority of urology patients, both men and women, believe that chaperones should be offered and that urological patients have the right to refuse a chaperone.8 The offer of a chaperone on its own is seen as a sign of respect for the patient in that chaperone-use becomes a patient-centered healthcare decision.5 Importantly, most patients within the broad scope of obstetrics and gynecology do not believe that the presence of a chaperone has negative effects on their appointment or relationship with their physician.5 These patients felt that a chaperone does not have a negative effect on trust in the doctor-patient relationship, does not break patient confidentiality, and does not cause embarrassment. This patient perspective may translate to the urology setting, but it requires further investigation.
Additionally, a small group of patients within the urology setting who do prefer the use of a chaperone during sensitive examinations still exists (Table 1). It is clear that the use of a chaperone benefits this group in particular, but further research needs to be done assessing what specific benefits are provided. From a broader perspective within obstetrics and gynecology, patients reporting about their breast examinations described feeling more at ease, more supported, and less embarrassed with a chaperone present during their exam.5 These benefits could translate to the urology clinic for patients who prefer chaperones. Particularly within the group of urology patients who do prefer to use a chaperone, there is also a subset of patients who do not feel comfortable requesting a chaperone if their physician did not offer one.9 These findings emphasize the importance of establishing standards of care which routinely offer chaperones during urological examinations.9
There are contradicting findings on chaperone gender preference. One study found that 93% of females preferred a female chaperone, whereas males were split between preferring female or male chaperones.7 Other studies within urology established that most patients did not care about gender of the chaperone, focusing more on comfortability with their provider and invasiveness of the procedure.8,9 Patients’ preference for a chaperone was not influenced by the gender or profession of the examiner.9 Another key finding is that the majority of patients prefer a chaperone to be either their family member or their friend.5,7 This preference opens new avenues for investigating patient preference regarding patient selection of a chaperone as well as determining who qualifies as a chaperone. These findings may determine whether or not current standard guidelines in chaperone-use are truly promoting patient-centered care and aligning with patient preference.
Many guidelines discussing the use of chaperones, including the AUA guidelines, promote the use of chaperones. Chaperones preserve patient dignity, increase respect, and build trust by creating a safe environment. Advocates of chaperones say they assist with privacy, interpreting instructions, and ensure that consent goes both ways and is continually being asked.10 Furthermore, advocates say they can ease anxiety among patients with cultural/religious backgrounds that may find a urological exam confusing and assist the physician by reinforcing their reliability.11 Patient trust is important; prior studies have demonstrated that those with less trust in their physician are more likely to report complaints that their needs or services were not met in an office visit.12
While patients believe that they should be offered the choice of a chaperone out of respect, many do not prefer to have one. This is an opposing view to physicians, who for the majority prefer the use of chaperones. A major reason for the physician sentiments is that physicians want to protect themselves from allegations and inappropriate conduct from patients. In one study, it was found that almost all physicians believe that chaperones protect both the patient and the physician. False accusations can damage a physician’s reputation and even possible legal proceedings.12 There is also a sometimes discordance between the patient and physician on who is best suited as a chaperone. It has been shown that 32% of patients prefer a chaperone that is their spouse/relative while 60% of physicians prefer the chaperone not to be related to the patient.12 This difference can cause both parties to feel uncomfortable, because physicians may not feel protected from legal issues that may arise because the chaperone is biased, while the patient prefers a relative for comfort and privacy given the sensitive nature of urology exams.
An issue that can skew actual chaperone use is physician documentation of chaperones. If physicians are not documenting their usage, then it is difficult to assess who is receiving chaperones. With proper documentation, it is easier to hire the right number of chaperones, delegate staffing, and increase efficiency by knowing which patients prefer chaperones beforehand. In one study, most physicians did not document the use of chaperones.13 In another study, it has been shown that interventions, such as adding a sticker or posters as reminders, done to motivate physicians to improve their documentation have resulted in more complete documentation. Post-intervention there was a 34.3% improvement in documentation of chaperone use and 22.9% improvement in describing the identity of the chaperone.14 Further studies must be done to determine the reason as to why physicians are not documenting chaperone use and what can be done to improve it.
Current clinical practice regarding chaperone use is not best aligned with patient preference because of gender biases. For example, male doctors are routinely chaperoned when performing an intimate examination on a female patient; however, 58% of women do not actually want a chaperone present.7 Men have also been reported to be victims of sexual abuse at the doctor’s office.15 The use of chaperones correlated with general practitioner gender, and male general practitioners were more likely to use a chaperone.16 The issue arises to prevalence as 90% of urologists are male and a majority of urology patients are male.10 There also appears to be more of an expectation that when a male performs a sensitive exam that a chaperone be present, while a woman physician does not have these same expectations.17 The majority of patients use chaperones for an intimate exam performed by the opposite gender and many physicians do not offer one if the patient is the same gender because of assumptions.18
Discussion
Many urologists have expressed concerns such as inefficient processes, inconvenience, and limitation on chaperone availability as reasons against their use.16 Guidelines and literature note that regardless of whether a chaperone is utilized, a patient’s decision comes first.4,5,18,19 Telehealth will require clear guidelines on the use of sensitive physical exams through video and audio platforms, indicating that the use of chaperones may need to be re-addressed to fall in line with the changing medical landscape.20 To increase efficiency, patient preferences for a chaperone can be clearly addressed during the scheduling process, which may accommodate staff availability in advance. For example, having a trained nurse present is associated with more frequent use of chaperones in clinic.17 In extenuating circumstances where chaperones aren’t available, it is nevertheless important to address patient preferences regarding the use of chaperones.
The medical community still is not clear about what should be considered standard practice regarding chaperone use in urology settings. Reasons include differing opinions between physician and patient opinion, lack of documentation, and gender biases as described above. Further research must be done specifically in the urology community as many studies involve gynecologists and general practitioners. This review focuses on capturing what is currently known about patient perspective on chaperone use through intimate examinations in urology, however, it is clear that more research investigating patient preferences might help elucidate how to modulate current clinical practice to fit best practice standards.
Conclusion
The utilization of chaperones during sensitive urologic examinations can be an important way to show respect to patients and to provide safety for both the patient and physician. Research suggests that the patient and physician perspectives differ regarding the purpose and role of chaperones in urologic examinations, as well as the preference of who will actually fill the role of chaperone during these examinations. While it is nearly impossible to optimize clinical practice standards to match the unique perspectives and preferences of each individual patient and provider respectively, the act of offering a chaperone prior to a sensitive urologic examination can build upon the patient/physician relationship, regardless if the chaperone ends up being utilized or not.