
Introduction
Over the past few decades, significant efforts have occurred toward gender equality in medicine. In 2017, 50.7% of medical school matriculates were women, outnumbering the proportion of men for the first time.1 Despite the trend of more women in medical school and in almost every specialty, a substantial gap remains in number of women vs men with leadership positions or senior rank.1–5 In 2017, only 37% of full-time anesthesiology faculty, 18% of full professors, and 11.5% of department chairs were women.6 Surveys from the American Society of Anesthesiologists also showed that women were significantly less likely to occupy leadership positions, participate in editorial boards, or speak on panels compared with their male counterparts.7
Authorship of peer-reviewed publications is important not only for residency and fellowship placement but also for academic rank and promotions.2 Research productivity may lead to numerous leadership and career opportunities.8 Whereas recent trends show substantial increases in female authorship, women are still underrepresented in research participation in many specialties, including ophthalmology, anesthesiology, general surgery, orthopedic surgery, neurosurgery, otolaryngology, critical care, dermatology, and dentistry.3,5,6,8–12 A study of over 1,000 peer-reviewed research articles in both surgical and medical specialties from 2000 to 2017 showed that women comprised 32% of first authors and less than 20% of senior authors.1 In anesthesiology journals, the proportion of female first authors increased from 20.5% to 30.2% from 2002 to 2017, and female senior authorship increased from 13.2% to 22.6%.6 These findings demonstrate substantial improvement but continued disparities.6 Studies from France, Canada, and the United Kingdom have shown similar inequalities in authorship of publications, suggesting that this pattern exists globally.10,12,13 Addressing gender-based inequalities in authorship of research publications is important, as it may have an impact on academic leadership opportunities for women in medicine.
Although the cause of the persisting gap in female vs male authorship is unknown, various theories have been proposed. Potential reasons include lack of mentorship and female role models, familial or home responsibilities, desire to maintain work-life balance, conscious or unconscious gender discrimination, and the increasing number of women in medicine has yet to increase authorship.5,10 Multiple studies have reported that female senior authorship was associated with increased likelihood of female first or coauthorship. This suggests the importance of woman-to-woman mentorship, particularly relating to research productivity and scholarship.3,5,6,14
To our knowledge, female authorship in pain medicine has not been studied. The objective of this study was to describe trends of female authorship from 2009 through 2019 in the 5 pain-medicine journals with the current highest impact factors.
Methods
Data Collection
We collected data for authors in the 5 pain-medicine journals with the highest impact factors, which were determined by searching InCites Journal Citation Reports (Clarivate) for “anesthesiology journals.” This search returned the names of 31 journals and their impact factor scores, from which we chose the top 5 for analyses: Regional Anesthesia and Pain Medicine (7.015), Pain (5.483), European Journal of Pain (3.492), Pain Physician (3.251), and Clinical Journal of Pain (2.893).
Peer-reviewed articles were evaluated for each journal from the following issues: January, April, and October in 2009, 2014, and 2019. For each article, we recorded the following information: journal name, journal month, journal year, article title or article PMCID, total number of authors, total number of female authors, total number of male authors, total number of authors of unknown gender, presence or absence of a female first author, and presence or absence of a female senior author. We considered the last author to be the senior author.
Gender was difficult to assess because consensus does not exist on a validated assessment tool.15 Given this situation, we used cultural norms for popular gender-specific names to determine the gender of each author, which were then assigned as either male or female. For names that were not gender-specific, an internet search was performed with the author’s name and affiliated institution to find a profile that included pronouns or photographs that identified the person as either a man or woman. If this search was unsuccessful, we used a gender probability calculator from the genderize.io website, which predicts gender based on a person’s name. Gender was only assigned if the calculator provided greater than 75% probability of a specific gender and if the count value (data rows examined to calculate the probability) was greater than 5. Any names with a gender probability less than 75% or a count value of 5 or less were recorded as indeterminate.
Data Analysis
We excluded 14 authors whose gender information was inadequate. In tabulations, we used number (%) for total female authors among all authors (with known genders) of articles published in that year. Because of the limitation that some female authors might be counted multiple times, proportions were used for data analysis. The difference in proportions of total female authors by year was assessed with mixed logistic regression models with random intercepts for each article. For all other variables, number (%) was used to represent count and proportion of articles; changes in proportions by year were assessed using the Cochran-Armitage test for trend. Data were averaged over the 3 years for comparison among the journals. We considered a P value of ≤.05 as significant.
Results
A total of 924 articles were reviewed (2009, n=284; 2014, n=326; 2019, n=314). Results for the number of female authors showed a nonsignificant upward trend (Table 1). From 2009 through 2019, the trend was toward fewer female first authors; however, the decrease was not significant. When men were the senior authors, women were the first author in 27.9% of articles (P<.001) (Table 2, Figure 1). In contrast, a woman was 2 times as likely to be first author when a woman was the senior author (57.2%) (Table 2, Figure 1), which points to the association of mentorship by senior female authors on junior female authors. Additionally, an article with 50% or more female authors was more likely to have a female senior author (76.4%, P<.001) (Table 2). When evaluated by year, these trends remained consistent and significant (P<.001).

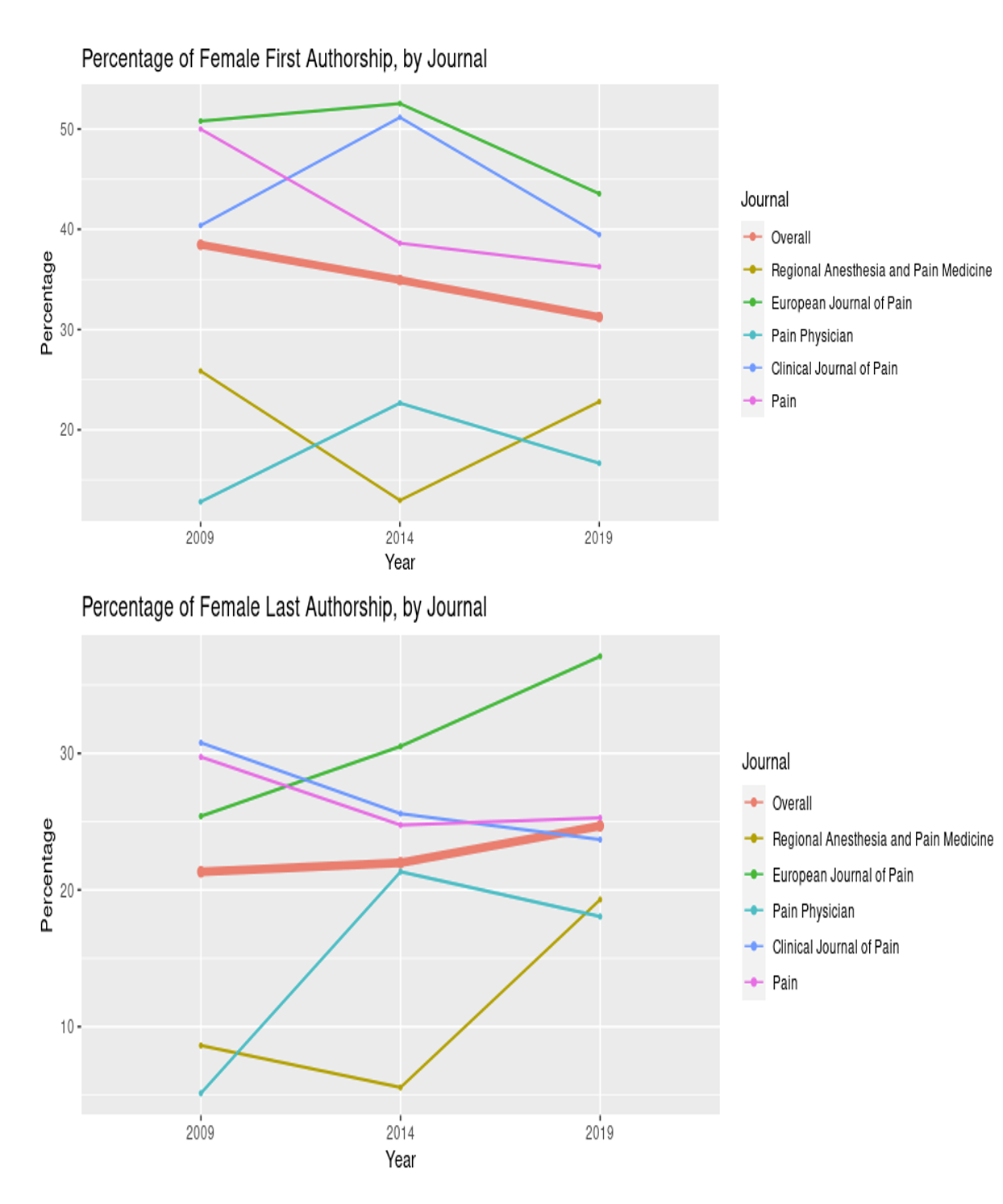
Our analyses of the averages over the 10-year period showed no differences in female authorship among the journals (Figure 2). Women comprised 20.7% of first authors in Regional Anesthesia and Pain Medicine. The proportion of senior female authors in Regional Anesthesia and Pain Medicine improved from 8.6% in 2009 to 19.6% in 2019 (Table 1). In the European Journal of Pain, women comprised 48.2% of first authors and 30% of senior authors (highest number of senior authors among the 5 journals). In the European Journal of Pain, 40.9% of articles had 50% or more female authors. The proportion of female authors in Pain Physician increased significantly from 9.8% in 2009 to 32.2% in 2019 (Table 1) (P<.001). In Pain Physician, women were first authors on 16.7% of articles and senior authors on 15.0%. Pain had 41.6% female first authors and 26.6% female senior authors, and 38.8% of articles had 50% or more female authors. In the Clinical Journal of Pain, women comprised 44.1% of first authors and 26.9% of senior authors.

Discussion
The study results showed little progress in the proportion of female authors over a 10-year period in the 5 pain-medicine journals with the highest impact factors. Similarly, female first and senior authors did not increase significantly over the decade. This stagnation mirrors the overall stagnation in female recruits to anesthesiology and, even more specifically, to pain medicine. Although women now make up a majority of medical students,1 they continue to be underrepresented as anesthesiology residents (35%), with little change over the last 15 years. Women are even more underrepresented as pain medicine fellows at 22%, which has not changed since 2009.16 Only 18% of pain-medicine physicians are women, which is proportionately less than in traditionally male-dominated fields such as orthopedic surgery and urology. Considering this low percentage, women were not underrepresented numerically as authors in pain-medicine journals, but, like the lag in recruits, the number of women authors is not growing. Reasons for the lag in women in pain medicine are similar to those for medicine in general and have been hypothesized to include reluctance of women to pursue fellowship (although other anesthesia fellowships accredited by the Accreditation Council for Graduate Medical Education attract women at much higher rates), concerns about work-life integration, exposure to radiation and risks to future fertility, and, most saliently, a culture perceived as unfriendly to women and lack of female role models and mentors in the field.16
In the journals we reviewed, women were about as likely to be first author as any author, but they were substantially less likely to be senior author. Given that senior authorship is often associated with later career achievement and promotion in academic rank,17 the underrepresentation of female authors at the senior author position is consistent with the so-called leaky pipeline, the now well-described phenomenon by which increasing representation of female medical students has failed to translate to higher proportions of women occupying the highest ranks of academia.18 Whereas women comprise 35% of the anesthesiology resident workforce and 36% of anesthesiology faculty, women hold only 14% of department chair positions and are half as likely as men to be full professors.19
Substantial differences were shown among journals in representation of female authors and in trends over the 10-year period examined. In Regional Anesthesia and Pain Medicine, women averaged only 20.7% of first authors from 2009 through 2019, whereas representation at the senior author position nearly doubled from 2009 (8.6%) through 2019 (19.4%). In contrast, women were first authors in 48.2% of manuscripts in the European Journal of Pain during the study period and senior author in 30.0%, the most representation among the 5 journals examined. The reasons for the discrepancies among journals are unknown but may include more women on journal editorial boards, specific diversity initiatives to increase female authorship, or author perceptions that some journals would be more receptive to manuscripts by women authors.20
Women were twice as likely to be first author on manuscripts with female senior authors than on papers with male senior authors. This finding agrees with findings of multiple studies from other disciplines that showed an association of female senior authorship with increased likelihood of female first or coauthorship.3,5,6,14 These findings suggest the importance of woman-to-woman mentorship, particularly relating to research productivity and scholarship. First authors are often early in their careers, and woman-to-woman mentorship for early career women in medicine is an important gateway to authorship and a stepping stone for research advancement. Conversely, our data revealed that male senior authors were only half as likely to mentor female first authors, compared with their female counterparts, which should be a call for male physicians in academic pain medicine to mentor their female junior colleagues.
Our study has limitations. We assumed based on our data that female first authors were being mentored by a female senior author, which may not always have been the case. In addition, the genderize.io website is not 100% accurate, and the possibility exists that gender was not correctly identified.
In conclusion, our results showed that women were less likely than men to be senior authors in the highest ranked pain journals and that no significant improvements for women as senior authors in these journals occurred in the last 10 years.
Acknowledgments
Marianne Mallia, ELS, MWC, senior scientific/medical editor, Mayo Clinic, substantively edited the manuscript. The Scientific Publications staff at Mayo Clinic provided proofreading, administrative, and clerical support.
Conflicts of Interest
The authors have no conflicts of interest to declare.
Funding and Competing Interests
None.
Authors’ Contributions
All authors made substantial contributions to all of the following: 1) the conception and design of the study, or acquisition of data, or analysis and interpretation of data, 2) drafting the article or revising it critically for important intellectual content, and 3) final approval of the version to be submitted.
Reprints
Natalie H. Strand, MD, Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, 5777 E Mayo Blvd, Phoenix, AZ 85054 (strand.natalie@mayo.edu).