Introduction
We are living in the COVID era. Since the outbreak of COVID-19, the endangered mental health of the global population across countries has led to COVID fear as there are significant increases in the level of anxiety, depression, post-traumatic disorder, and psychological distress.1–3 Given the adverse impact of COVID-19, it is highly possible that fear of COVID-19 would affect the attitude and intention for counseling. Surprisingly, however, there has been a lack of study to examine the possibility. In the current research, we would like to fill the gap by exploring the effect of the COVID fear on the attitudes and intentions towards the two modalities, online counseling and face-to-face counseling.
By definition, online counseling refers to mental health services provided via the internet while face-to-face counseling indicates the services delivered in person to the client. Before the COVID pandemic, online counseling has been considered an alternative or complementary modality for traditional face-to-face counseling,4–6 since it provides more convenience (e.g., easy access from home), privacy, and the relatively affordable fee of the service to the clients.7–9 Given the comparison, previous studies have focused primarily on the difference in evaluations of online versus face-to-face counseling. The results revealed that people tend to have a more positive attitude towards face-to-face counseling than online counseling.10–12 For example, March and colleagues11 reported in their community-based study that participants showed a higher preference for face-to-face services than for e-mental health services although they acknowledged their intention to use e-mental health services in the future when they have mental health difficulties.
During the COVID pandemic, however, online counseling emerged as a better option than face-to-face counseling for clients who have COVID fear because it enables them to get counseling with no physical contact with counselors in contrast to face-to-face counseling which requires physical contact.13–15 Thus, it is expected that the fear of COVID-19 would predict positive attitudes towards online counseling, while predicting negative attitudes towards face-to-face counseling. We further predict that the differential impacts of fear of COVID-19 on attitudes towards each modality would extend to intentions for each counseling given the well-established relationship between counseling attitude and counseling intention, relying on the theory of planned behavior.16
Overall, we hypothesize that the attitudes towards online and face-to-face counseling would differentially mediate the relationship between the fear of COVID-19 and intentions towards each counseling. Specifically, we expect that the fear of COVID-19 predicts positive attitudes towards the online counseling while predicting negative attitudes towards the face-to-face counseling. In addition, we anticipate that the contrasting attitudes between the two modalities will extend to the counseling intentions such that positive attitudes towards online counseling would lead to more intentions towards the online counseling, whereas negative attitudes towards face-to-face counseling would result in fewer intentions towards the face-to-face counseling. We did not have clear predictions regarding the direct effect of COVID-19 on each counseling intention. Given the robust negative associations of self-stigma and public stigma with attitudes towards counseling,17–19 we controlled both variables in our model.
Methods
Participants
We recruited 526 U.S. adult participants via Amazon Mechanical Turk (M = 29.82 years, SD = 5.14 years). Of those, 322 participants were women while 335 were White. All the procedures in this study complied with the principles of the Declaration of Helsinki, and all the participants signed an online voluntary-informed consent prior to study onset.
Measures
Unless otherwise instructed, participants indicated the extent to which they agreed with each item on a scale of 1 (strongly disagree) and 5, 6, or 7 (strongly agree).
Fear of COVID-19
We measured participants’ fear of COVID-19 with the 7-item Fear of COVID-19 Scale (e.g., “I am most afraid of coronavirus-19”) on a 7-point scale.20 Higher scores represent greater fear (α = .93).
Online Counseling Attitude (OCA)
We assessed attitude towards online counseling using the Online Counseling Attitude Scale (OCAS).21 The scale had 10 items, half of which measured the value of online counseling (OCA-V; e.g., “Using online counseling would help me learn about myself”) and the other half of which measured the discomfort with online counseling (OCA-D; e.g., “I would feel uneasy discussing emotional problems with an online counselor”). Participants rated each item on a 6-point scale. Higher scores of OCA-V represent a more positive attitude (α = .91), whereas higher scores of OCA-D represent a more negative attitude (α = .88). In the present study, participants were instructed to consider OC as the interaction with a counselor through the use of a secure video-conferencing platform (e.g., Zoom).
Face-to-face Counseling Attitude (FCA)
We measured attitude towards face-to-face counseling using the 10-item Face-to-face Counseling Attitude Scale (FCAS).21 5 items assessed the value of face-to-face counseling (FCA-V; e.g., “If a friend had personal problems, I might encourage him or her to consider face-to-face counseling”), whereas the other 5 items assessed the discomfort of face-to-face counseling (FCA-D; e.g., “I would dread explaining my problems to a face-to-face counselor”). Participants rated each item on a 6-point scale, with higher scores of FCA-V (α = .90) and FCA-D (α = .89) reflecting positive and negative attitudes, respectively.
Online Counseling Intention (OCI)
Behavioral intention to use online counseling was measured with four items (e.g., “I intend to use online counseling in the future”) as in previous research.22 Participants rated each item on a 7-point scale, with higher scores indicating greater intention (α = .95).
Face-to-face Counseling Intention (FCI)
Behavioral intention to use face-to-face counseling was measured with four items (α = .94), the same as online counseling intention. The only difference was that the term “face-to-face counseling” substituted for “online counseling”.
Covariates
Self-stigma was measured with the 10-item Self-Stigma of Seeking Help Scale (SSOSH), with items such as “Seeking psychological help would make me feel less intelligent”.23 Participants rated items on a 5-point scale. Public stigma was assessed using the 5-item Stigma Scale for Receiving Psychological Help (SSRPH), with items such as “Seeing a psychologist for emotional or interpersonal problems carries social stigma”.24 Each question was rated from 0 (strongly disagree) to 3 (strongly agree). Higher scores of SSOSH (α = .88) and SSRPH (α = .84) represent greater stigma.
Analytic strategy
To examine our hypotheses, we performed path analyses using Mplus, version 7.4 (ML estimation).25 A 5,000 bootstrapped resampling procedure was used to determine bias-corrected confidence intervals for the indirect effects. In all models, we controlled for the effects of self and public stigma on OCA-V, OCA-D, FCA-V, and FCA-D.
Results
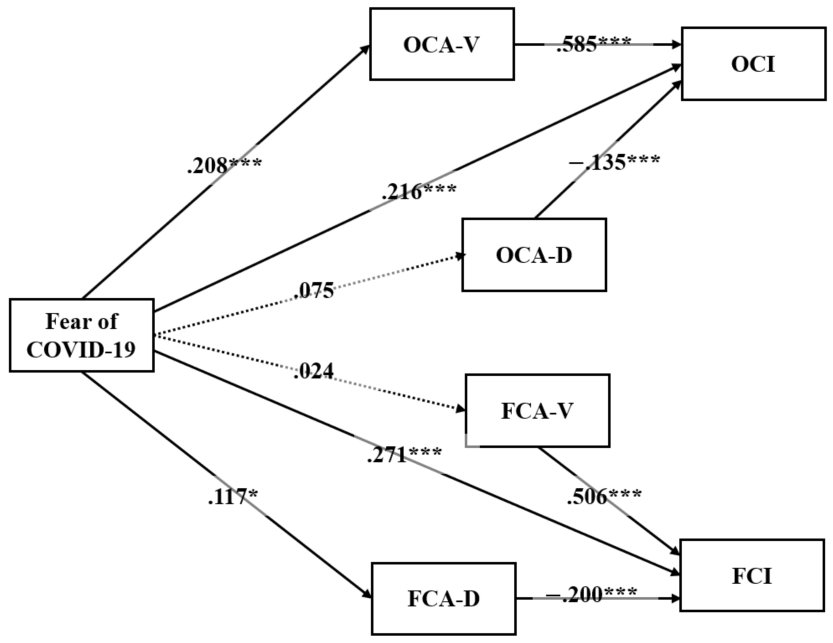
Descriptive statistics and correlations for all variables are reported in Table 1. We then conducted path analyses to test our hypothesized associations of fear of COVID-19 with attitudes and intentions towards online and face-to-face counseling, controlling for self-stigma and public stigma (see Figure 1). In our model, correlated errors among dimensions of OCA and FCA were permitted, given their significant associations with each other (see Table 1). We also allowed for correlated errors between OCI and FCI which were significantly related to each other (see Table 1).26

First, we tested a full mediation model (M1) with no direct paths from fear of COVID-19 to each counseling intention. In this model, dimensions of OCA and FCA were only linked with their corresponding counseling intention (i.e., OCA-V and OCA-D → OCI, FCA-V and FCA-D → FCI). Second, we tested a partial mediation model (M2) including the direct paths (i.e., fear of COVID-19 → OCI and FCI). Finally, the better fitting model between M1 and M2 was compared with a model (M3) in which the cross paths from OCA dimensions to FCI and from FCA dimensions to OCI were added.
The first model (M1) provided a poor fit to the data (10) = 102.475, p < .001; CFI = .948; RMSEA = .133 (90% CI [.110, .156]; SRMR = .055). On the other hand, the second model (M2) fitted reasonably well (8) = 26.139, p = .001; CFI = .990; RMSEA = .066 (90% CI [.039, .094]; SRMR = .021), improving model fit (∆(2) = 76.336, p < .001). The better fitting partial mediation model (M2) was therefore selected. We next compared M2 with M3. Although M3 provided an acceptable model fit (4) = 19.989, p < .001; CFI = .991; RMSEA = .087 (90% CI [.052, .127]; SRMR = .018), M3 did not improve model fit (∆(4) = 6 .150, p = .188). We thus retained the more parsimonious M2 (see Figure 1).
In our final model (M2), the results indicated that the direct paths from COVID fear to OCI = .216, p < .001) and FCI = .271, p < .001) were significant. Interestingly, each dimension of OCA and FCA was differently affected by COVID fear. Specifically, COVID fear significantly and positively predicted OCA-V = .208, p < .001), whereas it did not significantly predict OCA-D = .075, p = .065). In contrast, COVID-fear did not significantly affect FCA-V = .024, p = .552), whereas it significantly and positively affect FCA-D = .117, p = .003). The differential significant effects of COVID fear on OCA-V and FCA-D extended to OCI = .585, p < .001) and FCI = −.200, p < .001), respectively. That is, OCA-V mediated the relationship between COVID fear and OCI = .122, 95% CI [.075, .172]), while FCA-D mediated the association of COVID fear with FCI = −.023, 95% CI [−.046, −.008]).
Discussion
Although copious studies have documented the negative impact of fear of COVID-19 on a wide range of mental health,1–3 the impact on counseling intentions has received surprisingly little empirical attention. The present study bridges the gap by investigating the effect of fear of COVID-19 on counseling intentions via attitudes towards counseling, controlling for potential correlates. Our results showed that individuals with higher fear of COVID-19 had a more positive attitude towards online counseling (OCA-V), while they had a more negative attitude towards face-to-face counseling (FCA-D). Also, the contrasting attitudes between online and face-to-face counseling subsequently led them to have a stronger intention towards the online counseling and a weaker intention towards the face-to-face counseling, respectively. By verifying the novel pathways from the fear of COVID-19 to counseling intentions, the current work contributes to the COVID-19 literature as well as the field of counseling psychology.
It is worth noting that the direct paths from fear of COVID-19 to both online and face-to-face counseling intentions were significant and positive. In essence, the association of fear of COVID-19 with face-to-face counseling corresponds to an inconsistent mediation model. 27 That is, the direct effect of the predictor (i.e., fear of COVID-19) on the outcome (i.e., FCI) was directionally opposite to its indirect effect via the mediator (i.e., FCA-D). The results suggest that although individuals with high fear of COVID-19 want to get counseling regardless of its type, the negative nature of their attitudes towards face-to-face counseling might serve as a suppressor that holds them back from going to therapy. Thus, the current findings highlight the need to lower the entry barriers for potential clients by either emphasizing the positive aspects of online counseling (e.g., no need for physical contact) or underplaying the negative facet of face-to-face counseling (e.g., low risk of physical contact).
Despite the theoretical and practical contributions, we should note that the results are based on cross-sectional data, which does not imply a causal link between variables. Furthermore, the current data does not explain why the fear of COVID-19 is not associated with positive attitudes towards face-to-face counseling (FCA-V) and negative attitudes towards online counseling (OCA-D). More experimental studies on this topic are thus needed to corroborate our conclusion, with detailed accounts for the relationships among the variables based on relevant theoretical backgrounds.
Conclusion
The present study sheds light on the differential impact of COVID-19 fear on attitudes and intentions towards online and face-to-face counseling. Although the post-COVID era has been above the horizon, there may remain the individuals’ fear of COVID-19. As such, we hope our results would encourage further investigations on the possible determinants of the nuanced psychology of online and face-to-face counseling.
Author role
Jae Hun Shin and Xyle Ku served equally as lead for study design, formal analysis, and writing-original draft, review, and editing.
Acknowledgment
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request. This study’s design and hypotheses were not preregistered.