
INTRODUCTION
The outbreak of the SARS-CoV-2 virus in December 2019 gave rise to an ongoing global health crisis that has challenged nations worldwide to contain the spread of the COVID-19 pandemic. Nations have implemented varied campaigns to “flatten the curve” and control the pandemic through universal masking, social distancing, and efforts to isolate and protect those at higher risk of complications from the COVID-19 infection.1 The efforts were made in part to allow time for the development of the COVID-19 vaccines that will be instrumental in sustained long-term control of the COVID-19 pandemic. Early in 2021, formulations of the COVID-19 vaccine became available to healthcare providers and have been increasingly available to the general public in the United States.2
Evidence suggests that the initial BNT162b2 (Pfizer-BioNTech) and ChAdOx1-S (Oxford-AstraZeneca) COVID-19 vaccines have been overall safe and effective outside of their initial clinical trials.2–5 For example, an Israeli mass vaccination campaign utilizing the Pfizer–BioNTech product reported a relative risk reduction of 94%, corresponding to the relative risk reduction of the phase 3 trial (95%). However, the results indicated more vaccinations might be required to prevent one more case of COVID-19 than predicted in the initial clinical trial.5 Notably, despite new variants of the SARS-CoV-2 virus, studies suggest that the vaccines remain effective, albeit with reduced efficacy, underscoring the necessity of continued vaccine development and vaccination campaigns for long-term control of the COVID-19 pandemic.6
Vaccine hesitancy, defined as the behavior of delay in acceptance or refusal of vaccination despite availability, remains a substantial obstacle to effective long-term control of the virus.7 This stance is not isolated to the general public, as studies have shown this behavior extends to healthcare workers (HCWs) as well.1,8,9 Reluctance among HCWs may compromise public confidence in vaccination during an ongoing global epidemic. For example, studies have shown that HCWs are seen as trustworthy and credible sources of vaccine-related information.8,10,11 Hesitancy among providers extends to hesitancy in addressing the fears of their own vaccine-hesitant patients.8 Additionally, infections among HCWs, who are in direct contact with sick patients and thus at higher risk reduce the available healthcare workforce.11 We sought to identify statistically significant commonalities and differences among vaccine-hesitant HCWs to explore potential interventions that will be vital in both control of COVID-19 and future vaccination campaigns.
MAIN TEXT
Methods
Recruitment and Data Collection
Five hundred (N=500) healthcare providers (physicians, physician assistants, registered nurses, and nurse practitioners) ages 18 and over who chose not to be vaccinated were surveyed using a survey research platform that uses organic sampling built on Random Device Engagement (RDE).12 Using artificial intelligence (AI) to track unique respondent identification, RDE reaches users in their natural environments as they participate in their daily activities through any device. The survey platform’s partnership with over 120,000 applications and more than 700 million global users allows for random recruitment of participants fitting the specific inclusion criteria via in-app incentives particular to each user’s real-time activity on their respective devices.12 The advanced AI technology and algorithm prevent fraud from single users on multiple accounts and suspicious or illogical responses to specific questions. The survey platform uses weighting to match the univariate age, gender, and geographic region distributions. All results reported use this weighting.
Survey
We asked a total of 11 questions, including one screening question. The screening question inquired whether the survey-taker was a doctor, nurse, physician assistant, or nurse practitioner who chose NOT to receive the COVID-19 vaccine. The subsequent questions honed in on reasons for vaccine refusal, openness to accepting vaccination, and personal loss due to the virus, among other questions related to COVID-19 and vaccination. Participants also reported their age and gender, parental status, and other demographic variables. The survey instrument designed for this study can be found in the appendix.
Statistical Analysis
Data were analyzed using IBM SPSS Version 25 (IBM corporation, Armonk, New York, USA). Characteristics of the study participants and frequency of select survey responses were summarized utilizing descriptive statistics. To isolate possible predictors of vaccine hesitancy, we performed a multivariate logistic regression analysis using firm vaccine refusal (those who choose not to receive the COVID-19 vaccine and are convinced of their choice) as the dependent variable, with age, gender, the experience of death in family or friends from COVID-19, provider role, and parenthood selected as independent variables. Analysis was also performed on relative refusal (those who choose not to receive the COVID-19 vaccine but are open to being convinced with further research). All results used weighting to match the univariate distributions of age and gender.
Results
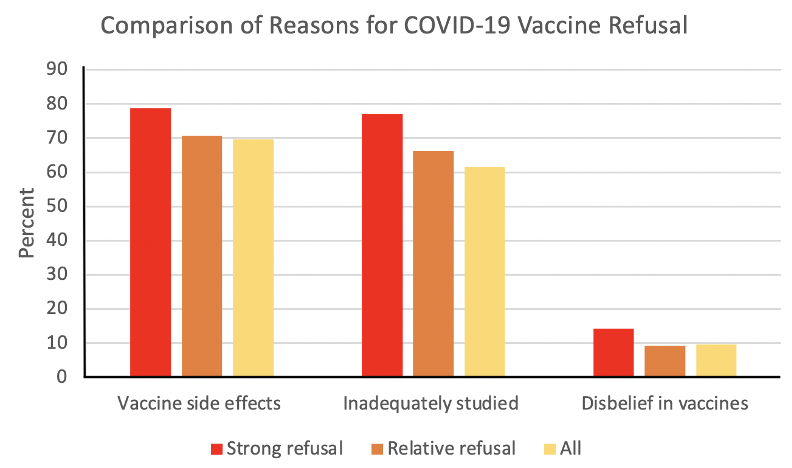
Due to the screening questions, all participants have chosen not to be vaccinated against the SARS-CoV-2 virus. A total of 225 males (45%) and 275 females (55%) made up the participant sample that included nurses (50%), physicians (24.8%), nurse practitioners (13.6%), and physician assistants (11.6%). Among the entire sample of HCWs choosing not to be vaccinated, the predominant reasons for vaccine hesitancy were a concern for vaccine side effects (69.60%) and the belief that the vaccines are inadequately studied (61.60%) (Figure 1). Disbelief in vaccines was a minority of answer choices (9.60%). Of those with strong refusal (n = 127, 25.4%), 78.74% were due to concern for side effects, 77.17% were concerned that the vaccine was inadequately studied, and 14.17% did not believe in any vaccines. Of those with relative refusal (n = 317, 63.4%), 70.66% were concerned about side effects, 66.25% were concerned that the vaccine was inadequately studied, and 9.15% did not believe in any vaccines.

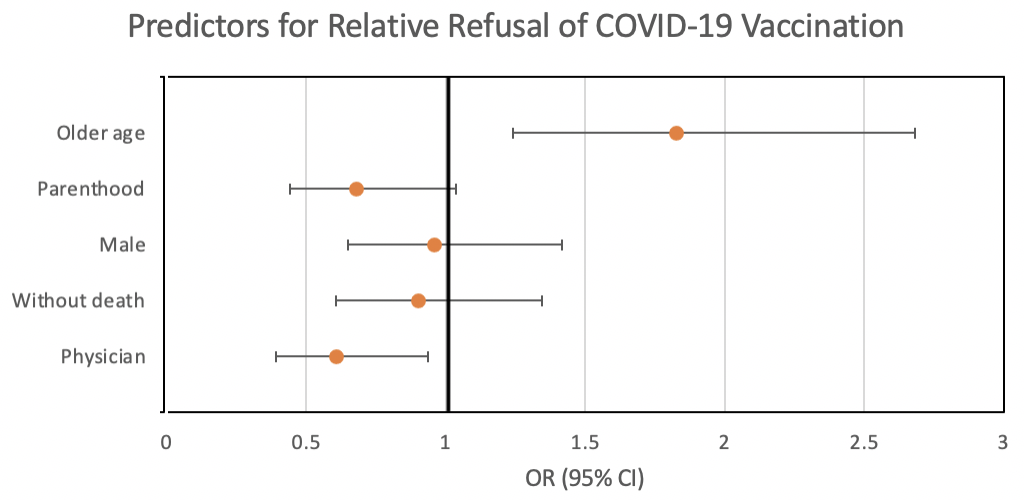
In the logistic regression analysis, several factors were independently associated with strong refusal of vaccination. Being a physician (OR: 2.64, 95% CI: 1.65-4.23, p < 0.001, parenthood (OR: 1.72, 95% CI: 1.05-2.81, p = 0.032), no family or friends lost to the virus (OR: 1.70, 95% CI: 1.06-2.72, p = 0.028), and younger age (18-34 vs 35 and up) (OR: 0.55, 95% CI: 0.36-0.85, p = 0.007) were associated with absolute refusal. On the logistic regression analysis, being a physician (OR: 0.61, 95% CI: 0.39-0.94, p = 0.025) and older age (35 and up) (OR: 1.83, 95% CI: 1.24-2.68, p = 0.002) were independently associated lesser and greater likelihood of weak refusal of vaccination, respectively.
Discussion
The availability of vaccination represents an important point in the global fight against the SARS-CoV-2 virus. However, vaccine hesitancy remains an issue among HCWs, who are both instrumental in vaccine acceptance among the general public and on the front lines of treating patients with COVID-19.8,10,11 Interestingly, our results suggest that among HCW choosing not to be vaccinated, being a physician is independently associated with a strong refusal of the COVID-19 vaccine (Figure 2). Previous studies on vaccine hesitancy have suggested that among physicians who choose not to vaccinate, reasons are multifactorial and complex. For example, hesitancy may be related to a perception of adverse effects, doubt about the efficacy of the vaccine, and a lack of trust in official sources of information.13,14 A component of physician vaccine hesitancy may also be related to personal practice experiences involving previous vaccines and their particular patient populations.14,15 Furthermore, the development of the first COVID-19 vaccines was uniquely mired in controversies of a rushed vaccine as well as a lack of trust in pharmaceutical companies and public health officials in a highly toxic political environment.2,9,16,17 These explanations correlate with other results from our survey that suggest that even among those with strong refusal, the vast majority had concerns regarding side effects and inadequate studies on the vaccine. In contrast, only a small minority did not believe in vaccines (Figure 1). It is important however to keep in perspective that these physicians represent an exceedingly small minority. As of January 2022, more than 96% of US physicians have been vaccinated against COVID-19, and of those who were not, most were planning to do so in the next few months.18

Our study also shows that among HCWs choosing not to be vaccinated, older age was independently associated with more openness towards further research studies to convince them of acceptance (Figures 2 and 3). Older age may be seen as a proxy for personal risk given the widely known increased mortality of COVID-19 in older age groups. Although an earlier report on COVID-19 vaccine hesitancy suggested that older age may be predictive of reluctance, the earlier report was conducted much earlier in 2020, possibly before disseminated knowledge of higher risk to the elderly.2,9 As expected, having no experience of death among close family and friends was also an independent predictor of strong vaccine refusal, which may be due to decreased perception of risk in those without personal loss to COVID-19.15,16 In our study, the aspect of risk also extends beyond personal risk, as being a parent was a statistically significant and independent predictor for strong vaccine refusal (Figure 1). This has also been demonstrated in previous studies and may be due to an increased fear of potential adverse reactions that may compromise the ability to care for one’s children in combination with the phenomenon of “omission bias,” where the decision to forgo. vaccination to avoid adverse reactions is reversible. In contrast, the opposite is untrue.1,15,16 However, parenthood may also correlate with less available free time to become vaccinated, better personal health, and reduced risk perception of contracting the COVID-19 virus.

An important objective of our study was to identify pathways toward reducing vaccine hesitancy among HCWs. Studies have shown that simple, direct vaccine advocacy campaigns may have a contradictory effect of strengthening vaccine hesitancy in specific populations, highlighting the need to adapt messages to specific vaccine hesitant groups.18 The use of multi-modal strategies that are culturally sensitive and personalized has demonstrated efficacy in reducing vaccine hesitancy when targeted at susceptible populations.11,19 For example, a combination of free and easy to access vaccinations, social media, and the involvement of religious or community leaders has shown effectiveness in addressing mistrust and physical barriers to vaccination.11,17–20 Vaccine hesitancy among HCWs presents a unique challenge given that vaccine refusal is complicated by multiple factors beyond simple denial of the science of vaccination (Figure 1). Based on our results, a multifaceted approach prioritizing older HCWs with risk factors while also addressing miscommunication and misunderstanding of potential disease severity among HCWs with children may have some benefits. Additionally, a more evidence-based and transparent approach promoting recent scientific evidence on efficacy and discussing the rarity of severe adverse reactions may be advised.3–5 Messages should be bereft of politics and presented with a focus on prosocial and emotional motivators - framing vaccination with altruism and the positive impacts of vaccination on family, close friends, and the wider community.17
The strength of our study is the focus on the differences among those who choose not to vaccinate as opposed to a comparison between those who vaccinate and those who do not. Studies have shown that a more targeted, personalized approach may be effective in reducing vaccine hesitancy, this study may help shine a light on potential interventions and future studies.11,19
Conclusion
Given the continued threat of an evolving SARS-CoV-2 virus, the issue of vaccine hesitancy will remain an ongoing concern.6 Our work suggests that hesitancy in receiving the COVID-19 vaccine remains a complex issue among HCWs that involves factors outside of simple disbelief in vaccines. There may be multiple avenues in addressing vaccine hesitancy through targeted interventions toward HCWs with COVID-19 risk factors and persistent promotion of the scientific evidence underlying the risks and benefits of vaccination.
Limitations
Although our survey utilized weighting to match univariate distributions of age, gender, and geographic region, response bias is inherent in survey research, which can be seen in the relatively young age of our respondents.12 HCWs who take the time to respond may also be those who have stronger opinions on the topic. Furthermore, the cross-sectional nature of our study cannot prove causality. Future research should continue evaluating the complex reasons behind vaccine hesitancy among HCWs. For example, qualitative interviews, larger analyses of specific subgroups of HCWs, and a more in-depth assessment of demographic characteristics may facilitate more targeted and effective approaches to vaccine promotion.19
DECLARATIONS
Ethics approval and consent to participate
HCA Centralized Algorithms for Research Rules on IRB Exemptions (CARRIE)/ IRB manager issued study exemption #2021-691. Survey respondents provided informed consent to participate in the survey.
Competing interests
The authors declare that they have no competing interests.
Funding
None
Authors’ Contributions
LG conceived and designed the study. DH and LG analyzed the data and designed the figures. DH and LG drafted the manuscript, and all authors contributed substantially to its revision.
Acknowledgments
This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.