
Introduction
COVID-19 is caused by a novel variation of coronavirus SARS-CoV-2 that originated in Wuhan, China late 20191 and subsequently spread to several countries with the first American case reported on Jan 21st, 2020.2 As of 4 December 2021, SARS-CoV-2 has subsequently evolved into several variants,3 and there have been over 265 million cases worldwide with over 5.25 million deaths. In the United States alone, there have been over 78 million cases with over 934,000 deaths as of February 20, 2022, associated with the virus.4
Coronaviruses are transmitted via respiratory droplets with incubation periods up to 14 days and have a wide range of presentations. Patients may potentially be asymptomatic, but may also display URI-type symptoms including fever, cough, sore throat, dyspnea, and malaise. Advanced disease is associated with multifocal pneumonia, acute respiratory distress syndrome, septic shock, coagulopathy, cardiac issues, and cardiac manifestations.5 Pediatric patients may develop pathology similar to adults, but may additionally have unique presentations that are often non-respiratory.6
Vaccines against SARS-CoV-2 are widely available to the public in the United States. The Moderna (mRNA-1273) and Pfizer/BioNTech (BNT162b2) vaccines currently have excellent safety profiles and have conferred 95%7 and 94.1%8 efficacy, respectively. Both have demonstrated a decrease in severe disease in vaccinated patients. The Pfizer/BioNTech (BNT162b2) vaccine continued to be efficacious over the course of 6 months with an efficacy rate of 91.3% a consistent safety profile, and high resistance to severe disease.9 The BNT162b2 and mRNA-1273 vaccines have additionally been tested on adolescents,10 with no serious side effects and similar efficacy to that of young adults, and thus are now available for children as young as 5 years old (12 years old at the time of this case).
Case Report
Ethical Considerations
The patient provided written informed consent for publication of this case report. HCA Centralized Algorithms for Research Rules on IRB Exemptions (CARRIE)/ IRB manager issued exemption 2022-036.
Case Presentation
This is a 15-year-old boy who presents to the emergency department due to a cough and shortness of breath. His mom is pretty sure he has COVID-19 pneumonia. She explains that her entire family has been afflicted with COVID-19. She says she just lost a cousin to COVID-19 last week. The patient’s symptoms started 5 days ago with anosmia, loss of taste, fever, headache, and dry cough. She suspected COVID-19 infection because her 3 older children, aged 25, 23, and 21, all got COVID-19 pneumonia and/or were hospitalized for it [Figure 1]. When his symptoms started 5 days ago, she immediately realized it was probably COVID-19 and did a telehealth visit. He was prescribed Ivermectin 21 mg daily for 5 days, dexamethasone 60 mg daily for 5 days, azithromycin, and a bumetanide inhaler. The patient has been taking medications as prescribed for the last 5 days but today he has been having difficulty breathing. The mother had a pulse oximeter at home and reported that his reading was as low as 88%. She has 2 younger children at home ages 12 and 6 who were also symptomatic. She herself is actively experiencing COVID-19 pneumonia. Nobody in the family is vaccinated. The patient does not have any medical or surgical problems, does not take any medications on a daily basis, and does not have any allergies.

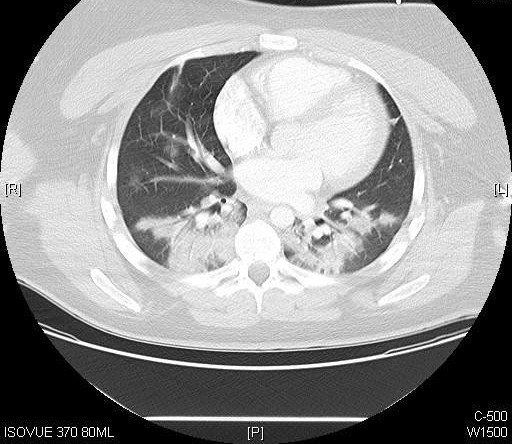
Upon arrival at the emergency department, his temperature was 98.9° F, pulse 70 beats per minute, respirations 26 breaths per minute, and blood pressure 126/71 mmHg. His oxygen saturation was 89% on room air. His basal metabolic index (BMI) is 31.9. Laboratory analysis revealed mild leukocytosis, bandemia, and metamyelocytes. His D-dimer was normal. Influenza and streptococcus screens were negative. Electrolytes were normal. Chest computed tomography scan revealed patchy bilateral upper and lower lobe ground-glass airspace disease consistent with COVID-19 pneumonia. No evidence of pulmonary embolism, aortic aneurysm, or aortic dissection was noted [Figure 2].

Electrocardiogram revealed a normal sinus rhythm with left axis deviation and nonspecific intraventricular conduction delay. The ventricular rate was 79 beats per minute, with a PR interval of 138 msec, a QRS duration of 102 msec, and a QTc interval of 440 msec [Figure 3].
The patient was given 10 mg of dexamethasone IV, azithromycin 500 mg IV, and 1 g of ceftriaxone IV as well as 1 L of intravenous fluids. The patient was admitted to the pediatric hospital for further management.
Discussion
This unfortunate case is consistent with COVID-19 pneumonia in a family that has been deeply affected by the same disease. The family had several members who were hospitalized and have even had a member who passed away. Our 15-year-old patient also received Ivermectin which does not have a strong evidence base.11 The rejection of vaccines in favor of treatments with no scientific backing behind them demonstrates a dangerous growing polarization that has resulted in the rejection of science as a whole and possible detriment to the sacred field of medicine. This polarization has likely also cost human lives in both those who believed the misconceptions and those who didn’t but were unable to get proper treatment or a hospital bed due to the overflow of people who did.
Surveys demonstrate that people who are directly affected by COVID-19 are more likely to pursue vaccination. Healthcare workers and people who have had family members contract COVID-19 typically had more positive attitudes toward vaccination.12 No one in the family had the vaccine despite its widespread availability and being free of cost. The mother explained that she did not want to put the children at risk of potential adverse effects of the vaccine and expressed concern about the potential for reproductive sterility.
Significant data has been gathered across many countries regarding vaccine hesitancy. Vaccine hesitancy was defined in 2015 by the WHO as a “delay in acceptance or refusal of vaccination despite the availability of vaccination services”.13 Vaccine hesitancy data have been multifactorial and fluid with time. Surveys demonstrated vaccine hesitancy in individuals with lower income and lower levels of education. In America, ethnicity played a role with black Americans having the highest amount of hesitancy. Homemakers and parents, as well as people in rural areas, were less likely to feel confident about vaccine administration.14 Levels of trust toward the COVID-19 vaccination have shifted with the stage of the pandemic. In April 2020 the worldwide rate of vaccine hesitancy was 21%. Three months later the rate climbed to 36% and subsequently fell to 16% in October of the same year.12
Personal beliefs about the vaccine, substantiated or not, play a large role in vaccine hesitancy. Wang et al. demonstrated that perceived susceptibility and severity of COVID-19 and perceived danger of the vaccine both affect individuals’ decisions to get vaccinated.14 These beliefs are exacerbated by conspiracy theories. For instance, according to a pew research poll, 71% of Americans have heard that the pandemic may be a planned conspiracy. More concerningly, of the group of people that heard the rumor, a third believe it may be true.15 A study that polled UK citizens shared the belief that 64% of the vaccine-hesitant believe that “the real truth about coronavirus is being kept from the public”.16 There are several sources of misinformation, with the largest source being social media contributes to 50% of fake news sources. Twitter and Instagram are common sources. Common fake news stories regarding COVID 19 include various false claims, conspiracy theories, and unsubstantiated cures.17,18
This case also highlights the infectivity of the virus, resulting in it affecting the entire household. The R0 number, or the reproductive number, refers to the average number of secondary infections caused by each new case of a disease.19 A lower R0 number thus indicates a lower chance of contagion and vice versa. The R0 number for COVID-19 is generally considered to be within 2.0-2.5,20 which means that for every person infected with COVID-19 who roams about freely, between 2-3 persons that said individual comes into contact with will get the infection. Although the R0 number for COVID-19 is less than those other infections such as measles, the seriousness of COVID-19 transmission is exacerbated by its asymptomatic prodrome, and the overlap of symptoms with infections such as the common cold.
Conclusion
The authors present the case of a 15-year-old boy who was infected with COVID-19 by his family and developed pneumonia severe enough to require hospitalization. This case illustrates the complexities of vaccine hesitancy and societal misinformation.
Disclaimer
This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.