On March 11, 2020, 70 days after the first media report of a ‘viral pneumonia,’ the number of global infections surpassed 118,000 cases, and authorities declared COVID-19 a global pandemic.1 Schools across the globe closed to slow the spread of the disease, affecting over 1.5 billion school-age children. With 194 countries reporting country-wide closures, 91.3% of all learners no longer were attending school.2 While being out of school may have protected individuals and communities from COVID-19, we must consider the impact of this and other disruptions on children’s lives.
While COVID-19 increases morbidity and mortality among older more so than younger people, this disease has impacted children and adolescents. During the stay-at-home situation, people experienced more significant household stress associated with fear of infection, food insecurity, and crowding.3 Most people worried about getting sick, but they were also concerned that relatives and friends would acquire and suffer from this virus. Children missed their classes, teachers, classmates, and friends. Besides complaints about boredom, children voiced anxiety over missing educational content, isolation from friends and family, and a general lack of control.3,4
During this same time, government and media sources offered messaging about COVID-19. Risk and crisis communication can offer diverse audiences information on best practices during public health emergencies.5 We know that coverage of the COVID-19 pandemic varied tremendously around the globe, with some countries providing news conferences and updating websites daily.6 Other governments downplayed the disease’s risk and failed to provide regular data on cases and fatalities.7,8 Also, media produced especially for children differed across countries.9
Children are a vulnerable audience. Effective health risk communication requires message receivers to understand, evaluate, and act on statistical information.10 During an emerging pandemic, news stories describe existing vulnerabilities and resources that can affect health.11 Given their stage of cognitive development and inability to comprehend abstraction, young children may struggle to make objective assessments of benefits and risks. Most have some difficulty distinguishing between labels like “possible” and “probable,”12 and many will have trouble understanding the likelihood of exposure.11 As observed with previous disasters, such as the Fukushima earthquake or the Iraq war,13 children develop inner pictures of the event based on regional media and public discourse.13–15
For some young people, acquired information can be protective; others experience short- and long-term negative consequences upon exposure to upsetting news reports.16 As COVID-19 significantly impacted children’s lives, this age group sought information and asked questions from different sources. A study done in Australia, Brazil, Canada, Spain, Sweden, and the UK revealed that children’s primary COVID-19 information sources were their parents/caregivers, TV, government websites, and social media.17 While there is ample evidence that children directly or indirectly seek out news information about manmade and natural crises,18 it is unknown whether the acquisition of knowledge calms or agitates children. During a crisis such as the COVID-19 pandemic, it is critical to understand better the impact of risk and crisis communication on youth. The objective of this analysis was to explore if and how children’s knowledge related to their concerns.
Considering data collected from a short but global survey done in Spring 2020, we had the opportunity to explore the relationship between children’s knowledge and concern about COVID-19. Were children who were more knowledgeable about the pandemic more or less concerned about the disease and its effects? Did this relation vary by geographic region? This examination offers important information to improve future crisis communication reaching preadolescents.
Methods
An international team developed and pilot-tested a 19-question online survey. Local teams announced the study through social media (predominantly Facebook and Twitter and listserves), and data collection occurred from March 31, 2020, to April 26, 2020. Several university committees on human research, including the University of Maryland Institutional Review Board (#1595915-3), considered and approved the study’s instruments and protocols. Both active parental consent and child assent were used.
We collected data from children between the ages of 9 to 13 years. In our analyses, we clustered data geographically, forming 8 regions from 42 countries.[1] Only countries with data from more than 50 children were included in the analysis. As cell sizes were extremely small for participants who did not provide information or identified as “other” for sex, we only included children who checked off boy or girl in our analyses. Given that group sizes varied, we statistically weighted the data by the number of participants, gender, age, and country.
The online survey had around 160 items, including demographics, COVID-19 knowledge, COVID-19 concerns, and sections about media use. (If readers wish to see the survey, they should contact the corresponding author.) To measure children’s knowledge about COVID-19, we asked 43 items about prevention and symptoms (Cronbach’s alpha= 0.62). Children received knowledge scores based on correct and incorrect responses about COVID-19. We gave children a score of +1 for a correct answer and -1 for a wrong answer.
We also assessed children’s worries about getting sick, family members and friends getting sick, missing classes and being out of school, and interruption of social activities. An overall concern score had 10 items and a Cronbach’s alpha of 0.76.
The analyses began with exploring univariate and bivariate relations around the different variables, considering significant associations at a p< 0.05 level. We looked at patterns within and between regions. We estimated regression models predicting overall and different types of concern, controlling for sex, age, and region (all of which were dummy variables). Into these models, we entered children’s knowledge about COVID-19 as well as an an interaction term between knowledge and region. Such an interaction term can tell us if the relation between knowledge and concern differed by region.
Results
Information on the final sample of 4,249 children appears in Table 1. We observed significant differences across regions. Children from the European sample had the highest mean knowledge scores, followed by North American and Asian children. Sub-Saharan children had the lowest mean knowledge scores but the highest scores for overall concerns. We found that children from Southeast Asia had the highest concern scores about getting sick themselves. Children from Asia reported the most significant worries about friends and family getting sick. Across regions, Sub-Saharan children were the most concerned, and European children were the least concerned about their schooling.
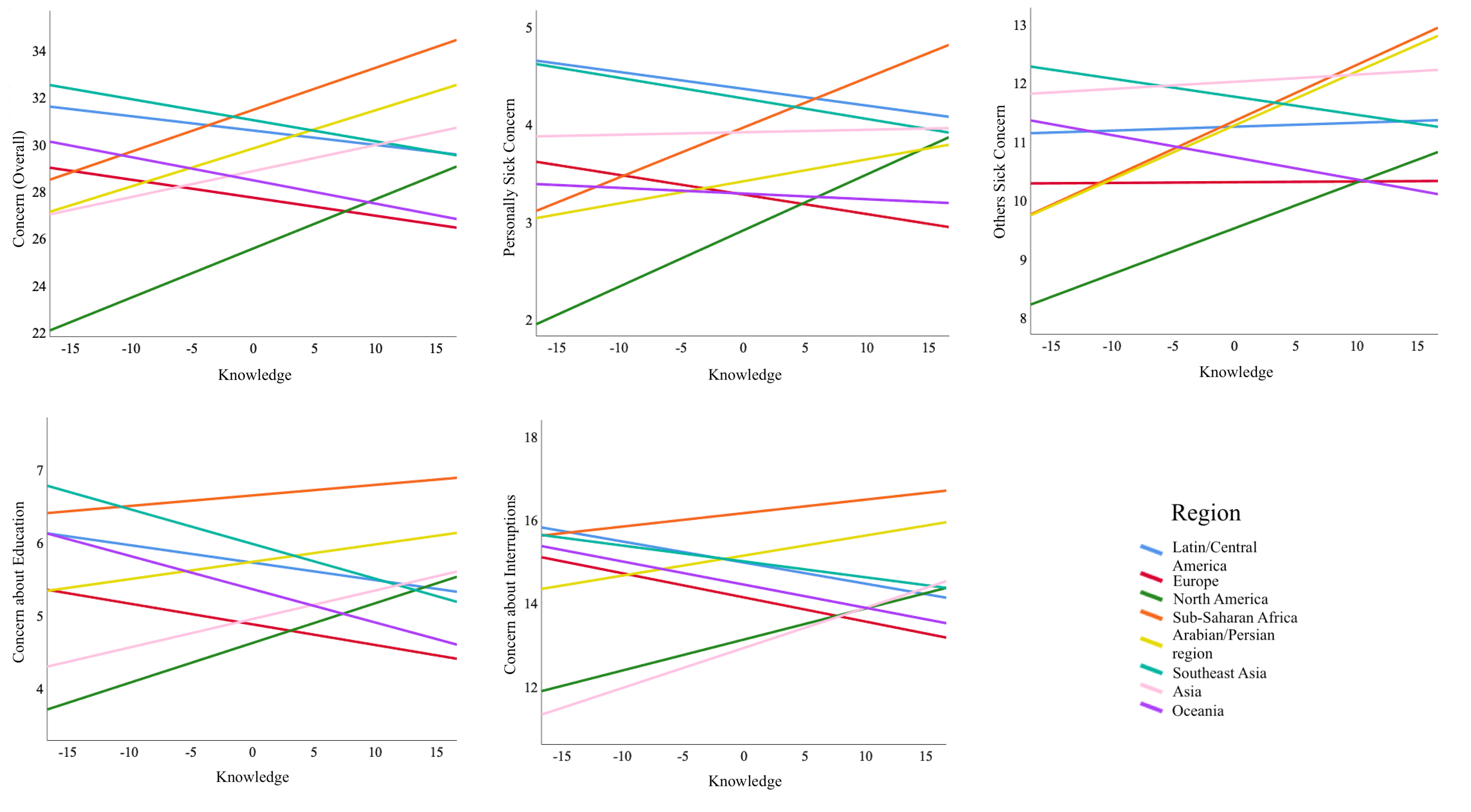
We estimated regression models, controlling for children’s sex, age, region, knowledge scores, and then looked at the interaction between knowledge and region. In all these models, the interaction term was significant, suggesting that the relation between knowledge and concern differed by region. Figure 1 shows the models predicting different types of concern where the slope reflects the interaction terms. Consistently, the relation between knowledge and concern was significant and positive among children from Sub-Saharan Africa, the Arabian/Persian region, and North America. In contrast, the interaction term was significant and harmful for children from Southeast Asia, Latin/Central America, and Europe, showing a relation where more knowledge was associated with less concern. Among children from Asia, we saw a positive relationship between knowledge and some but not all aspects of concern.

Discussion
Where a child lives not only affects their knowledge and concern about COVID-19, but also the relation between these constructs. In certain regions, including Sub-Saharan Africa, the Arabian/Persian region, Asia, and North America, children who had greater knowledge also had more concern about the disease. For these children, their COVID-19 knowledge was associated with more significant worry about personally getting sick, others getting sick, missing school, and interruptions to daily life. Among children from Latin America, Oceania, Europe, and Southeast Asia, the relation was flat or negative, suggesting that children from these areas who had more knowledge were less worried.
The observed global variation raises questions about how sources communicated and framed COVID-19 information. Conceivably, messaging around the origins, prevention, and symptomatology led to greater concern among children. In other locales, provided information may have eased children’s worries. It is also possible that children’s backgrounds and culture modified the processing of risk and crisis communication messages.19 This work suggests that children’s concerns vary and reflect differences associated with many factors including but not limited to the child’s media literacy skills, family background, socioeconomics and community culture. Such factors should be considered in developing media strategies and communication throughout a life cycle of a crisis.20
As this is a correlational study, we cannot assume causation or directionality in the observed relations. That knowledge and concern are significantly associated with each other does not mean that one causes the other; possibly a third factor causes increases and decreases in these two variables. For example, a country’s COVID-19 case and fatality rates might influence children’s information-seeking and concern levels. Additionally, we cannot specify the directionality between knowledge and concern. We can imagine that children’s knowledge levels exacerbated or placated their levels of concern. It is also possible children’s concern depressed or motivated information seeking, which would result in differential knowledge levels. As this study uses cross-sectional data, we cannot assume the directionality of the observed relation between knowledge and concern. In this study, we estimated models where knowledge predicted concern. Another reasonable analysis could have set knowledge as the outcome, where a child’s level of concern may have prompted his or her information-seeking or avoidance.
The study’s strengths include its broad reach and suitable timing. We successfully gathered a global sample during the peak period of school closures. A weakness, though, was recruitment occurred through social media and the Internet. This may bias the sample, with children from higher socioeconomic and more educated households being represented. Unfortunately, we have limited information on the participants’ demographics.
This study offers important insight on knowledge and concern during a public health crisis. A common assumption, especially among risk and crisis communication, is that more knowledge is better10,11; this may not be the case in specific locations and populations.
To better understand the relations depicted in this study, we need to evidence-based research of children’s current use and expectations of media20 as well as a content analyses of the disseminated messages. Such studies can inform best practices in producing risk and crisis communication, especially for children. As well, the field of crisis communication is shifting away from communications strategies that consider homogenous audiences.20,21 Especially for vulnerable groups, it is important that messages inform without creating greater concern.
An interesting finding from this study is that among children from European and Latin-American countries where public or state television offers children’s news and non-fictional current events programs, our data show a negative relation between knowledge and concern. In North America, Sub-Saharan Africa, and the Arabian/Persian regions, where very few or no regular children’s news programs exist,9 the relation between knowledge and concern was positive. As children desire and obtain news about current and even scary events, we recommend that producers create and broadcasters ensure the dissemination of news programs that cater to young people’s needs, interests, and developmental stages.18
Acknowledgments
Many people worked on the recruitment of children’s data, and we are grateful to the following researchers: Caroline Mendel, Dafna Lemish, Nancy Jennings, Rebecca Hains, Fatima Abdul, Meryl Alper, Hania Asgari, Hadiza Babayaro, Catherine Blaya, Sandra Cadavid, AnneLinda Camerini, Beth Carmona, Cynthia Carter, Mussa Chale, Mareike Düssel, Aldana Duhalde, Andria Gayed, Patricia Núñez Gómez, Macarena García González, Yuval Gozansky, Eileen Sanabria Herrera, Kirsten Huang, Liselot Hudders, Yisra Al-Haj Hussein, Hayuki Ishikawa, Ruchi Kher Jaggi, Colleen Russo Johnson, Andreas Klempin, Jennifer Kotler, Cheryl Kotwal, Geoff Lealand, Sun Sun Lim, Thomas Enemark Lundtofte, Mónica Maruri, Giovanna Mascheroni, Markus Mendel, Máire Messenger-Davis, Joél Mulongo, Diana Nastasia, Sorin Nastasia, Christina Ortner, Grace Torres Panganiban, Nilüfer Pembecioğlu, Martina Peštaj, Adrianna Ruggiero, Ulises Soto Ruiz, Isolde Stanczak, Jeanette Steemers, Fadi Taher, Sandra Téllez, Moses Tholley, Ekatarina Yakusheva, Andrew Zi Han Yee.
Contributions of authors:
Dina L.G. Borzekowski takes primary responsibility for this research and manuscript. She was part of the team that conceptualized the research, obtained approval from the IRB, assisted with data collection, managed the data analysis, and prepared the manuscript. Christopher R. Lane assisted with the data analysis and wrote up the manuscript. Maya Götz conceptualized and organized the global study from which this work was drawn. She also assisted with manuscript preparation.
Disclosure
The authors disclose that they have no conflict of interest with this research and paper.
Funding
The International Central Institute for Youth and Educational TV at Bayerischer Rundfunk (IZI) provided partial support for this work.
The groupings consisted of Europe (Austria, Belgium, Czech Republic, Denmark, France, Germany, Israel, Italy, Poland, Russia, Spain, Switzerland, Turkey, Slovenia, and the UK), Arab/Persian World (Egypt, Iran, Lebanon, Syria), Sub-Saharan Africa (Democratic Republic of the Congo, Nigeria, South Africa, and Tanzania), Southeast Asia (India, Malaysia, Philippines, Thailand), Asia (Japan, Singapore, and Taiwan), Oceania (Australia, and New Zealand), North America (Canada, and the USA), and Latin/Central America (Argentina, Brazil, Chile, Columbia, Cuba, Ecuador, Mexico, and the Dominican Republic).