Introduction
Sexuality is an essential part of a person’s life and plays a significant role in the quality of health and life in general.1 It primarily refers to sexual activity that is subject to change under the influence of experience and affects how a person sees themselves, their body, and sexual relationships.2 The presence of sexual dysfunction includes experiencing sexual desire disorders and physiological changes associated with loss of sexual desire and arousal, decreased sexual pleasure, difficulty achieving orgasm, anxiety, pain during intercourse, and loss of feelings of comfort.2 Due to advances in medicine and treatment, which have influenced earlier detection of potential cancers and improved patients’ survival, Emilee et al.3 report that the complexity of changes in female sexuality that can occur after a breast cancer diagnosis has been recognized. These changes often become one of the most problematic aspects, affecting different spheres of a woman’s life, can last for years after successful treatment, and in some situations, are associated with severe physical and emotional difficulties.3
Numerous researchers agree that the sexual quality of life of women with breast cancer is significantly impaired, implying that women faced with this cancer show a significant decrease in the frequency of sexual activity, the appearance of depressive symptoms accompanied by loss of sexual desire, menopausal symptoms, altered body image and dissatisfaction with appearance primarily as a result of mastectomy, changes in the relationship with the partner, and misconceptions about sexual relationships due to lack of adequate and verified information.4 Furthermore, a study conducted on a sample of sexually active women under the age of 50 showed that those women who underwent a mastectomy, possible breast reconstruction, hair loss due to chemotherapy, weight variation, poorer mental health, lower self-esteem were more dissatisfied with their body image and had a more significant misunderstanding of partners.2 It is a devastating fact that more than one-third of women with breast cancer develop a major depressive disorder, generalized anxiety disorder, or difficulty adjusting.5 Also, the cancer treatment itself causes several psychological effects such as lower self-esteem, body image disorders, decreased interest in sexual relations, and deterioration of personal and professional relationships that can lead to symptoms of depression.6
Sexual quality of life is an essential concern for women who have survived breast cancer.7 A study conducted on a European sample of newly diagnosed patients showed that 60% of women experienced changes in quality of sex life, of which quality was more impaired in women receiving chemotherapy, had a higher stage of the disease, were younger, and reported greater severity of depressive symptoms at the time of diagnosis and have undergone total mastectomy.7 In addition to the physical changes that accompany the onset of cancer, it is also essential to focus attention on the idea that women have about their sexual attractiveness and femininity because it has been shown that it is she who shapes the way she will perceive her illness and body.3
Although numerous modern studies support the recognition of sexuality as an essential part of women’s lives that is significantly affected by the diagnosis and treatment of breast cancer, to our knowledge, there are still few who address sexuality and give a more comprehensive overview of factors that can cause changes and reduce quality and pleasure. Given the realistic expectations about the reduced level of sexual quality of life in this part of the population, we hope that this work will help raise awareness of the changes that remain in the shadows that women and their partners have to face and suggest areas for health professionals to pay attention to. Also, with the detection of factors and the direction of their influence, specific measures can be taken, and more comprehensive psychotherapy interventions can be developed.
Women who are faced with breast cancer, and undergo various therapies, may experience significant changes in body image due to loss of body parts, scarring, skin removal, or various skin changes.8 Women who underwent mastectomy with breast reconstruction showed adverse changes in body experience and lower results in sexual life satisfaction but did not have significant differences in partner satisfaction.9 What is further worrying are indicators that women who are more dissatisfied with their bodies show higher levels of depressive and anxiety symptoms and lower self-esteem.10
Unfortunately, according to findings from various studies, more than 70% of women with breast cancer have depressive disorders that affect the choice and course of treatment and the outcomes of the disease itself.11 Research on women who have had breast cancer has shown a negative link between depression and feelings of femininity and body image, i.e., most women who felt less feminine and attractive reported a worse impression of their own body, showed depressive symptoms and were more dissatisfied with the quality of life as a whole.12 Understanding whether symptoms of depression related to the sexual quality of life more specifically would allow for more tailored interventions.
After initial diagnosis, depressive and anxiety symptoms are mainly in a downward trajectory.13 Namely, in a longitudinal study on an English sample of breast cancer patients, more than 50% of women developed depression, anxiety, or both years after diagnosis. This number was halved in the next three years.13 As with depression, environmental factors, such as lack of intimate social relationships, environmental support, the impact of previous psychological treatments, younger age, and exposure to significant stressors, have taken the lead in influencing duration.13 The area of female sexuality is mainly affected by anxiety symptoms, as suggested by research conducted on patients who were in remission for at least three months after treatment.14 The findings show that women generally reported poorer sexual functioning and decreased satisfaction, while sexual satisfaction and a negative body image were poorer in patients who experienced anxiety symptoms.14
Since the breast is an important cultural symbol of femininity and a part of the body that influences a woman’s self-esteem, lower self-esteem is considered a common consequence of cancer and its treatment.15 Self-esteem represents an evaluative and affective component of an individual’s self-view or a positive and negative attitude that a person forms about themself, their opinion, and behavior.16 Women who have changed their view of their own body due to different treatment methods show lower self-esteem.2 In a sample of women under the age of 50 who were married or in a stable relationship, Fobair and colleagues2 found a statistically significant association between self-esteem and body image, while the impact of self-esteem on partnerships and sexual functioning was not confirmed. Self-esteem is also associated with depressive symptoms, as shown by a study by Cieślak and Golusiński17 conducted on patients after mastectomy. The presence of depressive symptoms significantly reduced self-esteem in women. In parallel, the results of similar studies show a link between types of surgery, self-esteem, body image, and sexual life satisfaction.18 Patients undergoing sparing surgery were most satisfied with body image and reported higher self-esteem and sexual satisfaction compared to women who underwent mastectomy without reconstruction.18
Research has shown that partners play the most critical role in providing social support to women with chronic illnesses.19 Talley et al. found in a sample of women with early-stage breast cancer that emotional and instrumental support from partners was positively associated with the absence of depressive symptoms.20 Also, greater social support affects better sexual functioning and intimacy satisfaction in women who have undergone surgery in the past year, according to research by Kinsinger et al.19 Namely, women who perceived greater emotional and instrumental support from partners reported less sexual difficulties and greater satisfaction with intimate intercourse during all 12 months after surgery, while instrumental support showed the greatest associated with satisfaction immediately after surgery.19 Social support is a multidimensional construct encompassing emotional, informational, and instrumental support.19 These dimensions define the potential ways in which they support, which is extremely necessary for women with breast cancer, can be expressed. Emotional support involves empathy, active listening, receiving the comfort and love of loved ones, and informational support, including giving advice, guidance, and feedback on situations that concern us. Finally, instrumental support includes some kind of tangible help, such as help with children, household chores, paying bills, or taking care of therapy on time.19
The main objective of this paper is to provide a systematic review of research to determine the level of sexual quality of life in a sample of women with breast cancer with regard to grade, progression of underlying disease, types of treatment, body image, degree of depression, anxiety, self-esteem, and social support partners.
Method
To conduct a systematic review of the relevant literature to examine our aims, the PRISMA (Preferred reporting items for systematic review and meta-analysis protocols) method was used. The electronic databases used to collect the necessary literature (until August 2020) were PubMed, EBSCO, and Hack. The analysis included original scientific and review papers in English, published in the period from 2000 to 2020, and reviewed the bibliographies of all documents included to include further those not identified by the initial computer search. We chose 2000 as a starting point because a review of the PubMed database showed an increase in the number of published papers between 2000 and 2020, with 809 papers published in the last 20 years, while only 53 were previously found. Quality assessment ratings of the chosen papers were assessed by two authors (VK and LB). Quality rating items were adopted from previous literature that explored similar topics.21
The literature search strategy included the following terms and their combinations: breast cancer, sexual quality of life, body image, depression, anxiety, self-esteem, and partner social support (Appendix 1). These were also inclusion factors. Exclusion factors were all other cancers and psychotic illnesses in women with breast cancer.
The titles and abstracts of the publications obtained by this search were reviewed in detail. Further analysis included only those publications whose sample consisted of adult women diagnosed with breast cancer who were married or in a relationship to ensure those study participants were sexually active before cancer diagnosis. In this way, we can conclude how the diagnosis itself and its consequences influenced the perception of quality and satisfaction of sexual life. Furthermore, to determine the impact of partner’s social support in predicting the level of sexual quality of life in women with breast cancer, and to check the differences in the occurrence of depressive and anxiety symptoms depending on perceived support, it was important to unify the sample and only include women who were married or in a relationship. Furthermore, we excluded studies and data published only as abstracts and those that were repeated. As a final step, the entire papers of all potential studies were analyzed, and their inclusion was considered.
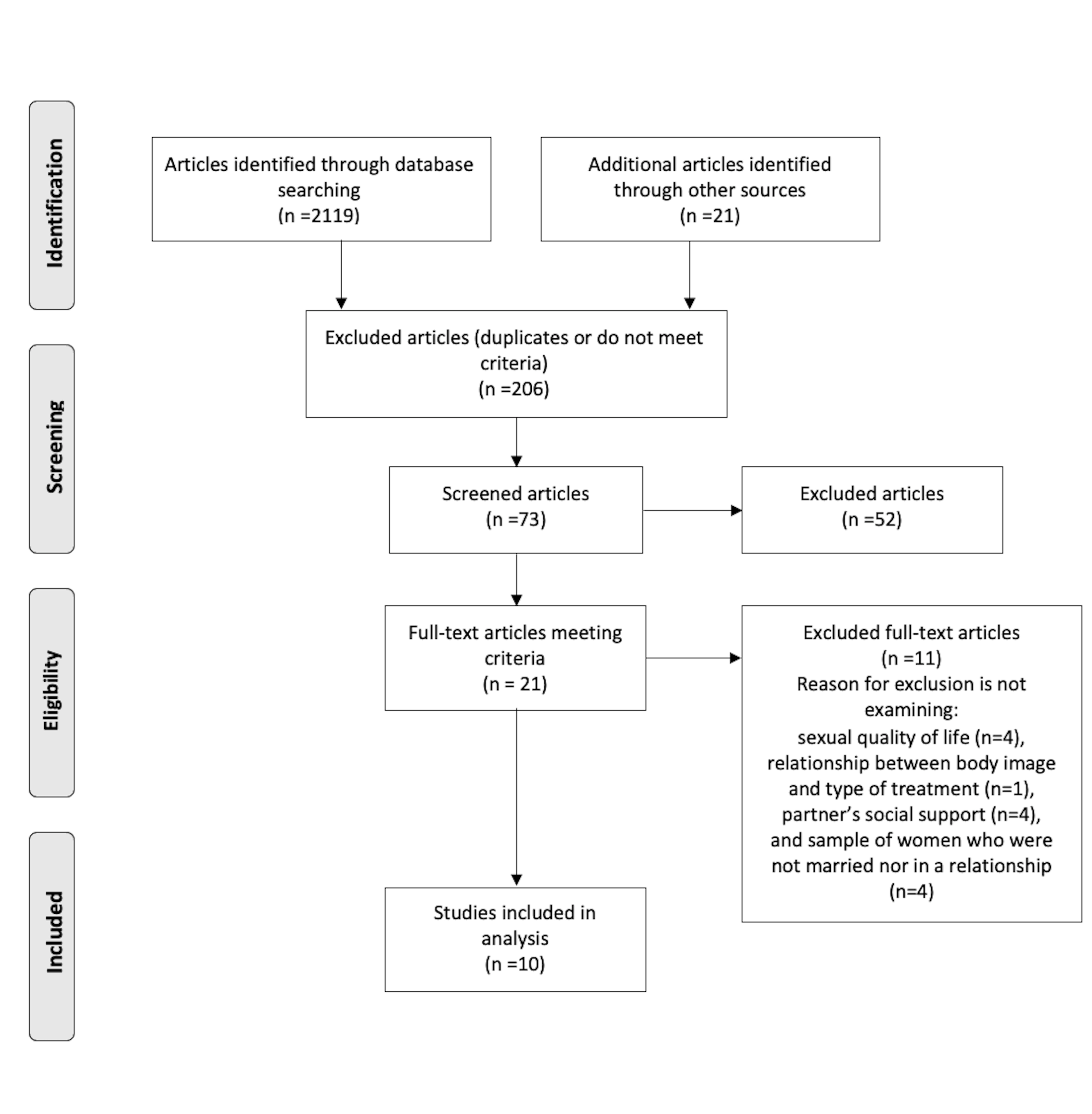
By entering keywords, a total of 2119 papers were detected, of which nine were included in the final analysis due to repetition and exclusion factors. A review of their bibliography highlighted an additional 21 papers, one of which was joined to the final analysis.
Results
After a systematic review of the aforementioned electronic databases using inclusion factors, the findings suggest that the sexual quality of life of women with breast cancer remains an exceptionally poorly researched area. What is particularly worrying is that a search of the Croatian portal Hrcak did not find any research that focused on sexuality and changes in its quality after the diagnosis and treatment of breast cancer in Croatian samples.
Figure 1 shows the course of the systematic review of the literature. The initial search identified 2119 papers, of which 2067 were excluded due to repetition and non-compliance with the criteria. This was followed by a review of abstracts that detected 21 relevant articles and included them in the detailed examination. Papers that potentially provide answers to the research questions were selected, their bibliography was reviewed, and we had nine scientific articles and one review paper in the final analysis.

The analysis includes ten papers published from 2000 to 2020 in the online databases PubMed and EBSCO. The first included study was published in 2006, while the remaining nine were published between 2010 and 2020. Most were longitudinal studies (50%), 2 cross-sectional (20%), one sequential (10%), one quasi-experiment (10%) and one review paper (10%). Considering geographical distribution, the United States (50%) leads in the number of included works. Two were conducted in Iran (20%), and one in France (10%), Turkey (10%), and the Netherlands (10%).
Table 1 shows the key characteristics of all ten papers, the main findings, and their conclusions. One study examined women’s sexual quality of life after treatment,6 while Den Oudsten et al.22 presented determinants that affect this aspect after surgery. Telli and Gurkan23 explained the effect of mastectomy on sexual quality and dyadic adjustment of women with breast cancer. A longitudinal study conducted in the United States examined the main and interactive effects that variables such as depression, treatment type, and cancer stage have on sexual quality of life.7 How sexual rehabilitation (PLISSIT model) affects the improvement of quality in sick women and their partners was also examined, and medical staff guidelines were provided.24
Furthermore, the frequency of changes in body image and the presence of sexual difficulties in the first months after treatment were determined,2 and factors influencing changes in body perception were categorized.25 Since partner social support has been shown to play a significant role in adequately coping with stressful situations such as cancer diagnosis and treatment, answers have been provided on the association of this construct with the severity of depressive and anxiety symptoms.20,26 In addition to quantitative analysis and interviews with patients, Canzona et al.27 took a step further in raising awareness of the factors influencing women’s willingness to talk openly about their sexuality to not go through a turbulent period on their own.
Table 2 shows the quality assessment ratings of the included studies. Eight studies met all criteria, while two studies did not report a rate of enrollment for participation. Across all studies, a total of 2,806 participants took part in the research, of which 2,287 were women with breast cancer, while 44 articles were included in the review paper. The sample size in each study ranged from 43 to 675, the youngest participant was 18 years old, and the papers do not specify the age of the oldest participant. The majority of the studies included married women or in a stable relationship (40%).
In comparison, descriptive data from a sample by Beckjord and Compas7 report 143 participants in a stable relationship (75%). Borstelmann et al.26 included 580 participants who met the criteria (86%). The French sample focused on women with an intimate partner or who have been sexually active in the last four weeks.6
The Sexual Quality of Life-Female (SQOL-F) scale28 was most commonly used to obtain data on sexual quality of life.23,24,27 Two questionnaires, the Short Index of Sexual Functioning in Women (BISF-W)29 and the Index of Female Sexual Function (FSFI),29 assessed the sexual quality of women with breast cancer in the last four weeks.6 The following two studies used the sexuality facet from the quality of life questionnaire as a relevant measure. The Dutch sample used the sexuality domain from The World Health Organization Quality of Life assessment (WHOQOL-100),30 composed of four items that show adequate reliability and validity with high sensitivity,22 while Beckjord and Compas7 used a subscale from the Cancer Rehabilitation Evaluation System, Short Form (CARES-SF)31 composed of 3 items.
Sexuality is the most disrupted quality of life in women with breast cancer.7 Studies using the SQL-F recorded significant sexual quality deficits in a sample of women with breast cancer in Turkey, the United States, and Iran. Women who underwent mastectomy after diagnosis achieved a significantly lower score (M = 43.3, SD = 29.4) compared to the control group (M = 80.1, SD = 21.4).23 Similar findings were obtained by Canzona et al.,27 and according to them, patients with breast cancer face impaired sexual quality daily (M = 53.4).
No statistically significant difference was obtained with regard to disease progression (MI = 56, SD = 9.3; MII = 52.6, SD = 6.3; MIII = 49.9, SD = 95.1; MIV = 57, 5, SD = 3.8) or exposure to hormonal therapy (MDA = 53.7, SD = 5.9; MNE = 54.6, SD = 5.5).27 A study on an Iranian sample measured the sexual quality of life of affected women and their partners on two occasions: before and after rehabilitation.24 Before conducting sexual rehabilitation, 87% of participants rated sexual quality as poor, yet there was no statistically significant difference between experimental and control groups (X2 = 0.003, p > .05) while after attending rehabilitation, an increase in satisfaction was measured in the experimental group.24
The combination of BISF-W and FSFI with the French sample under the age of 35 after treatment did not show more optimistic results. The average total score of sexual functioning (BISF-W) was 28.08 (SD = 15.87), which indicates a reduced quality compared to the healthy population (p = .030), and the differences were significant in sexual arousal (p = .017), enjoyment (p = 0.002) and pleasure (p = .002).6 The results on FSFI did not show discrepancies between the mentioned groups (M = 25.14, SD = 8.09; p < .01).6 Also, the types of therapy in treatment did not result in significant changes in sexual experience.6,22
Furthermore, time is an important factor that affects the reduction of quality of sexual life (M1 = 15.21, SD = 3.1; M2 = 14.4, SD = 3.27; M3 = 14.17, SD = 3.41; M4 = 14.03, SD = 3.17, M5 = 14.08, SD = 3.47; p = .002) as evidenced by the findings of Den Oudsten et al.22 Self-esteem, body image and depression did not contribute to the explanation of sexual quality (β = -0.12; β = -0.04; β = -0.12), while higher severity of anxiety symptoms explained the decrease in this domain (β = -0, 12).22 In contrast, the results of a longitudinal study on a sample of 191 patients showed the highest positive association between sexual quality of life and depressive symptoms (r = .47), followed by cancer stage (r = .24) and age (r = -.19).7 Women treated with chemotherapy were more dissatisfied with their sexual quality of life (M = 1.96, SD = 1.15) and reported more pronounced depressive symptoms compared with women undergoing mastectomy (M = 1.67, SD = 1.22).7
Invasive breast cancer therapies cause major physical changes and leave consequences on a woman’s perception of her own body. A study conducted in the USA found that more than half of the women occasionally experienced at least two disorders in body image, of which the most common are feelings of less femininity (55%) and concern for sexual attraction (53%).2 The disorders were most pronounced in persons who underwent mastectomy (R = .67, p <.05) and chemotherapy (R = -.51, p < .05), during which they lost hair and faced changes in body weight and who faced a partner’s misunderstanding of feelings (R =.23, p < .05).2 Furthermore, an association between self-esteem and body image disorders was demonstrated in a way that women who experienced physical disorders showed lower levels of self-esteem.2 In parallel, Rezaei et al.25 reviewed 690 articles to identify factors that affect body image and classified them into four categories. Among the bio-psycho-socio-economic factors should be mentioned anxiety, depression, self-esteem, and a sense of shame for the body. The following categories include cancer progression, duration and treatment modalities, various physical deformities, and sexual functioning.25
Borstelmann et al.26 and Talley et al.20 recognized and explored the importance a partner may have in providing social support to a woman with breast cancer. Women who rated their partners as supportive perceived higher social support (MS = 89.6) and showed fewer symptoms of anxiety (MA = 7.2), compared to women who assessed that their partner did not support them (MS = 75.9; MA = 9.2).26 The manifestation of depressive symptoms also proved to be significantly related to social support. Hence, the results in a sample of women undergoing radiotherapy suggest that the emotional support of partners significantly reduces the persistence of depressive symptoms. In contrast, instrumental support did not prove statistically significant.20
Discussion
Since it has been shown that due to the diagnosis and coping with the consequences of breast cancer, a woman’s sexual quality is more impaired than other quality of life domains,7 the importance of detecting and understanding specific factors influencing its variation was emphasized.
Even though one in every four women diagnosed with cancer has breast cancer,32 research on patients’ sexual quality of life is still underdeveloped. After a thorough and detailed examination, we were able to detect only seven papers that focused on examining changes in the most affected aspect of quality of life in women who have been diagnosed with this cancer at some point in their lives.2,6,7,22–24,27 All seven studies found that women with breast cancer reported a statistically significant impairment of sexual quality of life, consistent with initial assumptions. Namely, the more time that passes from the initial diagnosis, the quality becomes smaller unless the woman is encouraged to talk openly about the problems she is facing and gets involved in various rehabilitation programs.
Most research has included medical data, thus determining how much the underlying disease’s progression affects sexuality. Unfortunately, we do not have grade data, so although a higher grade suggests a more aggressive type of cancer and a worse prognosis, we cannot conclude how it affects the sexual quality of life. Previous research has shown how the development of the cancer stage changes difficulties that patients face and their daily existential worries and needs. Thus, research by Hamer and colleagues33 showed that women with metastatic breast cancer report lower levels of all domains of quality of life, and face higher levels of pain, sleep disorders, loss of appetite, and more pronounced symptoms of depression and anxiety compared to women with earlier-stage cancer. Given that most previous psychosocial interventions have focused on helping to adapt and accept cancer, understanding the specific requirements of women depending on the stage of the disease would help health professionals adapt and create specific support programs tailored to unique needs that depend on the stage of the disease. Also, since the type of treatment depends on the progression of the disease, these findings could serve as guidelines in advising patients when planning medical interventions.
Moreover, inconsistent results were found regarding disease progression. Beckjord and Compas7 Research showed a significant positive association between cancer progression and sexual quality of life. Other findings did not confirm that the type of cancer causes significant changes in quality. Such discrepancies are possible because the sample of women was not unified, i.e., not all women in the samples were married, or in an intimate relationship, some studies focused exclusively on women under 35, and patients were exposed to different types of treatment that we assume to have a more significant impact on quality in general. In addition, other questionnaires and scales were used to assess the sexual quality of life that have different psychometric characteristics. Hence, discrepancies in findings could be caused by different methodology approaches. Another aspect worth noting is cultural differences that could have played a role in assessing the sexual quality of life. Other countries have different stances regarding women’s expression of satisfaction or dissatisfaction with the sexual quality of life. Thus, finding should be interpreted cautiously, keeping in mind these cross-cultural differences.
Types of treatment have proven to be extremely important in terms of sexuality and the way a person perceives and feels about their own body. Research agrees that much support is needed for women who have undergone surgery, i.e., total mastectomy, and have faced the consequences of chemotherapy such as hair loss and weight changes.2,7–9 Women after mastectomy and chemotherapy talk about dissatisfaction and changes in sexual life and do not look at their body as a source of femininity and attractiveness, which confirms hypotheses and falls in line with the results obtained by Gopie et al.,9 Hopwood et al.,8 and Kostov and Tucak Junaković.34 In other words, mastectomy and chemotherapy cause the most significant reduction in a woman’s sexual quality of life and poorer body image, while changes in the cognitive, subjective, and behavioral aspects of the body cause a decrease in femininity and attractiveness, less sexual activity, and less enjoyment and sexual pleasure. It would undoubtedly be helpful to examine the effects of each treatment in more detail and see which aspects of a woman’s life are endangered to select the treatment that will yield the best results while preserving the patient’s physical and mental health.
Unfortunately, almost no attention has been paid to the level of self-esteem in women with breast cancer, even though its impact has been confirmed in previous research. Only two studies that looked at which factors best predict the sexual quality of life22 and examined changes in body image and sexuality,2 in addition to the overview of factors influencing the image of the body,25 included this construct as a variable related to sexual quality and body image, which changes under the influence of treatment. It has been shown that women who report lower levels of self-esteem have an impaired quality of sexual life and a more negative attitude about their own body, which confirms our expectations. Also, mastectomy and chemotherapy have proven to be crucial in women’s negative attitudes towards themselves. Women with higher levels of depression and anxiety reported reduced sexual quality. However, no consensus was reached on whether either disorder had a more significant impact, which would be desirable to examine in future research. The presence of these symptoms depended on whether women felt they were getting enough support and understanding from their partners. Again, in line with assumptions and previous findings, more signs were associated with insufficient backing. In addition to being extremely demanding to deal with diagnosis and treatment, women also deal with the fear of being rejected and unwanted by their partners. If they feel that their partner does not understand them, does not support them, does not find them attractive and desirable, they will be less likely to engage in sexual relations, and their quality of sexual life will suffer. Canzone et al.27 went a step further. They showed how readiness to discuss this issue can be crucial in raising quality and singled out those areas that hinder patients, on which health professionals can base their intervention. Future research should further explore the association of level of sexual quality of life in women with breast cancer and other crucial areas of everyday functioning to find ways that could contribute to better coping and adjustment of patients to diagnosis and treatment, but also useful in educating partners about specific procedures that would facilitate the process and improve mutual satisfaction with the intimate relationship.
Limitations and further implications
Although a detailed and systematic review of the available literature with regard to inclusion factors has been carried out, the possibility is not left out that some relevant papers were skipped or remained unrecognized during the review of abstracts. Additional electronic search databases, such as PsycINFO, Sciences direct, would find new research that would lead to new insights. The limitations also lie in the included samples. Apart from the fact that most of the research conducted in the USA and the samples differed significantly in size, not all sampled women were married or in an intimate relationship, which is why we need to generalize their results to the population with caution. The question also arises as to whether, with an increase in the sample in some studies, some associations would be obtained that were not currently statistically significant.
Given that the review of the papers confirmed the importance of sexual quality of life in women with breast cancer, we believe that this construct should be investigated in more detail and compare the population with women who do not have cancer. It would be essential to see how the diagnosis, development, and treatment itself affect the quality and moderate the relationship between body image, self-esteem, and sexuality. Given the impaired sexual quality of life that comes in high comorbidity with anxiety and depression in patients, the findings could serve as a reasonable basis for creating psychosocial interventions that would improve recognition of different emotional states and teach women new coping mechanisms. Given that the intimate partner is a significant source of social support for women facing consequences of cancer, it is implicated for researchers to explain the impact further that emotional, instrumental, and informational support have on various aspects of life and how they reduce the development of the disorder. Given the above, the focus of psychotherapy could be to improve interpersonal relationships to prevent the onset of the disorder and educate partners on how they can make it easier for women to cope with a serious illness and improve their quality of life.
Conclusion
Research indicates a statistically significant association between sexual quality of life and type of treatment, while no data on the effect of grade were found. Of the types of treatment, the most consequences are caused by mastectomy and chemotherapy, which, in addition to quality, also affect the change in body image and the level of self-esteem in patients. The association between sexual quality of life, body image, depression, anxiety, self-esteem, and social support of partners was also shown. Women who have changed their view of their bodies due to their diagnosis and treatment are considered less feminine and sexually attractive and are less likely to have sex. Furthermore, they are less confident compared to women who have not undergone mastectomy and chemotherapy. Anxiety and depression most often come in comorbidity and reduce the sexual quality of life in women with breast cancer. The increased incidence of depressive and anxiety symptoms is also influenced by the partner, who is the most important source of support in dealing with a serious illness. Women who perceived insufficient social support from partners were less satisfied with the quality of sexual life and had more pronounced symptoms of depression and anxiety.
Contributions of authors
Lovorka Brajkovic – work designed; acquisitions and analysis and interpretation of data; drafting the work; literature search, final approval of the version to be published; Agreement to be accountable for all aspects of the work
Petra Sladic - acquisitions and analysis and interpretation of data; drafting the work; literature search, final approval of the version to be published; Agreement to be accountable for all aspects of the work
Vanja Kopilaš – conception of the work; revising the work; analysis and interpretation of data; final approval of the version to be published; Agreement to be accountable for all aspects of the work
Conflicts of interest
There are no conflicts of interest.