Introduction
Sensory and motor impairments often result in cognitive decline that affects physical movements. Physical functioning entails a broad spectrum of activities ranging from basic self-care to more intricate tasks that demand balance, strength, endurance, and other abilities.1 In such situations, movements may need to be controlled and performed at an associative or cognitive level. This can make the postural control of older adults more susceptible to cognitive distractions.2 Recent studies have uncovered that executive functions can mitigate the consequences of motor and sensory impairments on falls.3 Executive functions are essential for everyday tasks that require attention, cognitive actions, rapid motor planning, and effective executive skills. Regrettably, as we age, it becomes increasingly challenging to maintain multiple task rules in our working memory, which can lead to difficulties with executive function.4
Many forms of alternative healing, especially those based on working with energy, have not been fully proven to date. Blessing/Biofield therapies are one type of non-pharmacological intervention (NPI) that falls under complementary and alternative medicine (CAM) therapies. Several research studies have demonstrated the efficacy of biofield therapy in reducing anxiety and pain, promoting muscle relaxation, aiding in stress reduction, promoting wound healing, and improving overall health and quality of life in humans.5–10 Biofield therapy encompasses various practices that promote healing and enhance overall wellness. These practices include Reiki, Therapeutic Touch, Qi Gong, and other energy healing methods that aim to rebalance and optimize energy flow within the biofield.11,12 By addressing imbalances in the body’s subtle energy systems, biofield therapy can alleviate physical, emotional, and psychological distress. The manipulation of the body’s subtle energy field is a fundamental aspect of biofield therapies, which promotes relaxation and restores balance.13
According to the existing literature, only a limited number of studies have investigated the use of distant biofield energy treatment for managing various diseases or symptoms.11,14–18 Distant healing intention involves the use of various form of remote biofield energy therapy (RBET), such as blessing, therapeutic touch, Reiki healing, external qigong, spiritual healing, and prayer. This refers to a deliberate and conscious mental effort aimed at improving another person’s physical or emotional well-being from a distance.19 RBET, also known as virtual biofield energy therapy, takes place via phone, electronic app, video chat, etc. These options allow people to seek treatment in the comfort of their homes without traveling to see a healing practitioner in person. Proponents of RBET claim that it promotes healing by exchanging or channeling energy beyond the physical realm. However, there has been no study to demonstrate the effectiveness of distant biofield energy/blessing therapy on cognition and motor function performance in adult subjects. Therefore, the authors would like to observe the effectiveness of remote (distant) blessing therapy (R/DBT) in improving human cognitive-motor functions. One of the theories is quantum entanglement theory, which suggests immediate physical correlations over large distances.20,21 This theory proposes that subjective mental activities, such as conscious awareness, can interact with reality in ways that the brain cannot.22 This suggests that DBT is a non-local phenomenon.23 The hypothesis for this study is that this therapy stimulates different areas of the brain, leading to improvements in cognitive and motor functions. It is assumed that blessing energies are transmitted to the central nervous, autonomic nervous, immune, and endocrine systems, which could potentially influence the entire human body. This study is based on the hypothesis that distant blessing energy therapy (DBET) has the potential to impact the human body in various ways.
This study aimed to examine the use of distant blessing/biofield energy therapy as a non-pharmacological intervention (NPI) remotely to improve neuropsychological and physical functioning in adults with self-perceived neuropsychological impairments. The researchers used cognitive and motor subsets of the NIH Toolbox® to assess neuropsychological outcomes.
Materials and Methods
Study design
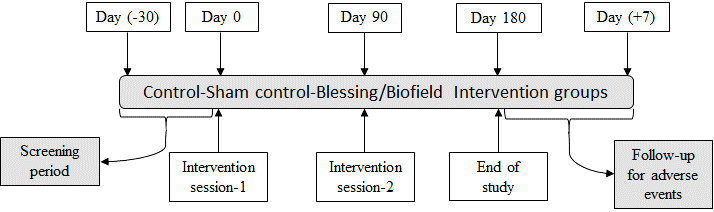
This study involved a randomized, placebo-controlled, double-blind, three parallel groups, single-center trial. A total of 168 subjects were screened, and 135 subjects meeting eligibility criteria were enrolled (1:1:1 ratio) in order to achieve 117 completed subjects. The enrolled subjects were assigned to three different groups viz. control, sham control, and biofield intervention as per randomization process. The control group (naïve) participants did not receive any intervention/treatment throughout the study periods for a particular condition. The remote procedure was followed for the control group participants, but without any spiritual healer or other person. Besides, the sham control group subjects were received treatment remotely by a “sham person”, who did not have any knowledge about the energy healing concept from United States of America. All the enrolled subjects were followed until end of the study. Data were assessed at three time points i.e., randomization/baseline/first session treatment (day 0), second session treatment (day 90), and end of study (day 180) (Figures 1 and 2).


Study ethics
Good Clinical Practices and the Declaration of Helsinki were followed during the conduct of the study.20 The clinical study protocol, informed consent document, and all other relevant study documentation were reviewed and approved by the Institutional Ethics Committee (IEC) of Riddhi Medical Nursing Home, Gujarat, India (ECR/886/Inst/GJ/2016/RR-19). The study involving human subjects were approved by the Clinical Trials Registry – India (CTRI) with the clinical trial registration number CTRI/2022/07/043736.
Randomization
After evaluation of screening parameters, receipt of a signed informed consent and order of the investigational therapy for each subject equal allocation of the sequence was ensured. Each of the three groups was randomly selected from the eligible subjects viz. control, sham control, and biofield intervention group (1:1:1) with the help of simple randomization technique. An allocation concealment mechanism was applied to generate the random allocation sequence numbers using SAS software (v9.4; SAS® Institute Inc., Cary, NC, USA). The randomization schedule was maintained under controlled access. The personnel (statistician) involved in the distribution of investigational therapy was accountable for ensuring compliance to the randomization schedule.
Blinding
This study was double-blind meaning that the treatments were blinded to the subjects and principal investigator. In this study, the treatments were done remotely at day 0 and day 90 to the participants. However, the staff involved in laboratory procedures and collecting objective data were blinded to the subjects under evaluation to maintain the study integrity.
Sample size justification
In order to estimate the sample size required, an a priori power analysis was conducted. The treatment groups were predicted to have an effect size of 0.8 based on Cohen’s d. The total number of participants required to find an effect was estimated to be 105, assuming a power of 80%, an alpha error rate of 5%, and a drop-out rate of 10%. Enrolled participants were assigned into three groups using SAS software.
Criteria for inclusion and exclusion of participants
Prior to enrollment, all subjects were screened by the principal investigator for eligibility. Briefly, our inclusion criteria were: South Asian population (India; male and female) with age of 20 to 55 years; subjects complaint with cognition deficits related symptoms (situations of uncertainty, unable to make right decisions, unnecessary and negative thought coming without intention, difficulty in remembering things, etc.) and motor deficit related symptoms (physical weakness, tired, fatigue, etc.); body mass index (BMI) should be 18.5 to 35.0 kg/m2, calculated as weight in kg / (height in meters)2; female participants of childbearing age agreed to use acceptable forms of birth control during the study; agreed to provide written informed consent and able to follow the study directions to participate in the study and complete all follow-up; and agreed to comply with the study requirements and procedures as per study protocol. Our exclusion criteria were: past history within last one year or currently having alcohol dependence or drug abuse; significant diseases or clinically significant abnormal findings in medical history, physical examination, laboratory evaluations, etc., during screening; regular vigorous aerobic/endurance exercise (>3 vigorous bouts/week); known history of positive HIV, HCV, HBsAg, or VDRL/RPR; subjects with non-healthy, non-homogenous, damaged over the skin; subjects with birthmarks or excessive hair over the skin; subjects with the usage of self-tanning agents for at least ten days before screening; and female subjects who demonstrate a positive pregnancy test or currently breast-feeding or planning pregnancy.
Withdrawal criteria
The investigator might withdraw a subject from the study for any of the following reasons: (a) if the subject withdrew his or her self-consent for any reason; (b) if the subject’s condition had worsened to the degree that the investigator feels, it was unsafe for the subject to continue in the study; (c) if the subject has taken any medication; (d) if an adverse effects occurred for which the subject desired to discontinue treatment or the investigator determined that it was in the subject’s best interest to be discontinued; (e) if there was any types of significant protocol deviation; (f) if a concomitant therapy was reported or required which was liable to interfere with the results of the study; (g) if the subject was lost to follow-up; and (h) administrative reasons.
Participant adherence and engagement
The principal investigator used an effective engagement strategy based on the usability data and user feedback as per the study protocol. At every visit time, the participants were intimated over mobile and SMS to visit the research center for intervention and data collection, which directly enhanced the adherence to individual engagement. Each and every precaution was taken into consideration before taking any data from the participants. Self-reported symptoms with real-time self-monitoring of moods and behaviors and participation in the NIH Toolbox® experiment of each participant were recorded in the electronic case report forms (eCRF).
Distant Blessing/Biofield energy intervention strategy
The eligible subjects were assigned to the control (no intervention), sham control (sham person) and biofield energy intervention group. The biofield energy intervention group subjects received two sessions of distant/remote blessing/prayer (biofield energy treatment) by a renowned spiritual healing practitioner on day 0 and 90, under the standard clinical laboratory setting. The healing practitioner has been practicing biofield energy healing therapy for more than 8 years and regularly blessed the clients. The Blessing/Biofield Energy Healing Therapy (Trivedi Effect®) was administered remotely/distantly from Washington, United States of America using the zoom.us platform, channeling universal life force energy for about 5 minutes to a group of mass volunteers at a time in Cliantha Research Limited, Ahmedabad, Gujarat, India. The healing practitioner harnessed the subtle energy (thoughts and emotions) from the universe through her unique ability and transmitted universal life force energy into the subject’s body in the blessing treatment group via laying her hands. The client’s energy work takes place within their subtle anatomy, which encompasses the aura and chakras. The client simply receives the energy and doesn’t need to do anything special. The practitioner focuses energy by imagining a connection to a universal life energy source. Practitioners are not required to ascribe to a particular religion; they simply need to believe that there is a higher power or universal life energy that can be focused on healing clients. Besides, the sham control group subjects also received a placebo kind of attunement from a sham person in a similar manner so as to nullify the baseline responses. The start and end time of distant healing was recorded in the electronic case report forms (eCRF). All the participants, including remote biofield energy treatment group subjects, were seated silently in a room at Cliantha Research Limited. They can’t see each other during treatment sessions, because black tape tied with their eyes. The participants did not see the sham person/healers.
Safety Assessment
An adult population was selected in which chances of interference of concurrent diseases were very unlikely and various safety-related parameters (adverse effects, medical history, physical examination of vital signs) and laboratory assessment (hematology) were performed. Our previous publication had already established the safety profile of biofield energy treatment on human population.5,6 Using the MedDRA (Medical Dictionary for Regulatory Activities) terminology allows for consistency and standardization in the classification of adverse effects.24 Before study therapy all current and past diseases and their respective treatments was recorded.
Physical examination of vital signs
Physical examination of vital signs such as blood pressure and pulse rate (Digital Pressure Meter, Omron Healthcare Co. Ltd., Vietnam), respiratory rate, and body temperature (Digital Thermometer, Nureca Limited, USA) was performed at the time of screening, randomization/treatment (day 0), treatment (day 90) and at the end of treatment (day 180), in order to evaluate the adverse effects if any. Before evaluation of vital signs individuals were informed to remain seated during the experiment for about 5 minutes.
Hematological parameter
Different safety-related hematological parameters such as erythrocyte sedimentation rate (ESR; mm/1 hour), hematocrit (HCT; %), hemoglobin (g/dL), mean corpuscular hemoglobin (pg), mean corpuscular hemoglobin concentration (g/dL), mean corpuscular volume (fL), platelet count (10^6/L), total RBC count (10^12/L) and total WBC count (10^6/L) in order to evaluate the adverse effects. All the hematological parameters were measured using Sysmex XN-550 hematology analyzer, Sysmex Corporation – Japan.
Assessment of Cognitive and Motor Functions Using NIH-Tool Box Test Battery
The NIH Toolbox® is a reliable and versatile computer-based assessment tool that covers a variety of domains, including cognitive, emotional, motor, and sensory functions.25,26 It’s great to hear that the National Institutes of Health supported the development of such a comprehensive tool for assessing neurological and behavioral functions.26 When it comes to the cognition section of the NIH Toolbox® provides a specific neuropsychological instrument battery that helps to probe several cognitive domains such as working memory, episodic memory, attention, executive function, processing speed, language, and reading.27 In addition to that, motor function was also identified as a critical domain for inclusion in the NIH Toolbox®, given its importance to overall neurologic health and function. The NIH Toolbox® motor battery includes five subdomains, namely locomotion, dexterity, balance, strength, and endurance, which are all essential for monitoring and maintaining motor function.28 A test battery system has been recommended to assess different subdomains, including the 9-hole peg board, standing balance test, grip dynamometry, 2-minute walk test and a 4-meter walk test. These measures are valid, reliable, low-cost, and portable. Moreover, this test battery system has several advantages, such as applicability across the age span, psychometric soundness, ease of use, and applicability in diverse settings.29 The subdomain structure was selected as per study protocol. Through this process, 6 subdomains were identified as the most relevant areas of cognition functioning: language, processing speed, working memory, episodic memory, executive function, and attention. Moreover, 5 subdomains were identified as the most relevant areas of motor functioning: locomotion, standing balance, dexterity, grip strength, and endurance.
Cognitive function
The trained investigator performed all the cognitive assessments using the NIH Toolbox® Cognition Battery (NIHTB-CB, Version 1.25.6068) application.30 Three test versions were used to reduce practice effects and were administered in random order for each participant. The NIHTB-CB tests 6 fluid cognition subdomains (language, processing speed, working memory, episodic memory, executive function, and attention) to yield a fluid cognition composite score.31 The NIH Toolbox® Picture Vocabulary Test Age 3+ v2.1 for the evaluation of cognitive language ability in a computerized adaptive format.32 The individuals are provided with an auditory record of a word and four images on the computer monitor. The task is to touch the image that most closely indicates the word’s meaning. High-resolution color photos were selected from the Getty Images library and were used as stimuli. Participant performance was converted into a picture vocabulary theta score (+4 to -4), as per item response theory.33 Processing speed was evaluated using “NIH Toolbox® Pattern Comparison Processing Speed Test Age 7+ v2.1”. Here, task was given to the individuals to identify whether two visual patterns are “same” or “different”. The responses were taken by pressing a “yes” or “no” command. The visual patterns were either identical or variable in dimensions: color, adding/taking something away, or one versus many.34 Working memory was assessed using “NIH Toolbox® List Sorting Working Memory Test Age 7+ v2.1”. In this test, participants were asked to identify which of four pictures reflects a specific word and scores were noted based on the number correct.35 Episodic Memory is the capacity for storing and retrieving information, is critical for the acquisition of knowledge and for building adaptive skills. This test is susceptible to a variety of diseases like encephalitis, temporolimbic epilepsy, and Alzheimer’s disease.36 This test is based on nonverbal pictorial stimuli that must be placed in a predefined sequence, with increasing numbers of pictures for older age groups.37 In this study, authors used NIH Toolbox® Picture Sequence Memory Test Age 8+ Form A v2.1 for the assessment of episodic memory. The NIH Toolbox® Dimensional Change Card Sort Test Age 12+ v2.1 for the assessment of executive function (cognitive flexibility) and NIH Toolbox® Flanker Inhibitory Control and Attention Test Age 12+ v2.1 for executive function (inhibitory control). The NIH Toolbox® Flanker Inhibitory Control and Attention Test Age 12+ v2.1 was adapted to assess attention. Flanker task can identify the orientation of the stimulus presented at the center of the screen while ignoring surrounding stimuli (flankers) that could be incongruent. Inhibiting attention to the flankers is crucial for accurate responses. In the traditional flanker task, the stimuli are arrows pointing left or right.38
Motor function
All of the motor evaluations were carried out by the same trained specialist using the NIH Toolbox® Motor Battery (NIHTB-MB, Version 1.25.6068) program. The assessment included five subdomains, which are crucial for optimal motor function across the lifespan, namely locomotion, standing balance, dexterity, grip strength, and endurance. The NIH Toolbox® Motor Battery emphasized the evaluation of gait speed while walking on a flat surface using the NIH Toolbox® 4-Meter Walk Gait Speed Test Age 7+ v2.0.39 Additionally, the NIH Toolbox® Standing Balance Test Age 7+ v2.0 was employed to evaluate balance. The 9-Hole Pegboard Dexterity Test Age 3+ v2.0 was used to assess the ability to manipulate objects with precise finger movements. The NIH Toolbox® Grip Strength Test Age 3+ v2.0 (electronic hand dynamometer, Levipil) was utilized to evaluate grip strength.40 The raw score is commonly utilized for interpretation, with greater force (in pounds) indicating greater strength. For the NIH Toolbox® Motor Battery assessment, the fully corrected T-score is the score that should be primarily utilized for interpretation, as it considers differences in gender, age, ethnicity, and education. Lastly, the NIH Toolbox® 2-Minute Walk Endurance Test Age 3+ v2.0 is recommended for inclusion in the NIH Toolbox® Motor Battery. This test is easy and safe for administration to individuals across the age span from 3 to 85 years.41
Statistical Analysis
In the descriptive analysis of the sample, continuous variables were expressed using the mean, median, and standard deviation (SD) for normal distribution. For continuous variables, the p-value was calculated using Analysis of Variance (ANOVA), and for categorical variables, the p-value was calculated using the Chi-square test. The data were represented as the mean ± standard deviation/standard error of the mean (SEM) and were subjected to statistical analysis. The statistical analysis of the NIH-TB-CB/MB test score (prior correction from the baseline, CFB) was performed, and the level of significance (p-value) was determined using one-way repeated measure Analysis of Variance (ANOVA) followed by post-hoc analysis by Tukey’s test with a 95% confidence interval (CI) of the difference between treatments using SigmaPlot (v14.0). The statistical analysis of the NIH-TB-CB/MB test score after CFB was performed, and the level of significance (p-value) was determined using one-way repeated measure Analysis of Covariance (ANCOVA) with a 95% confidence interval (CI) of the difference between treatments using SAS® 9.4 (SAS Institute Inc., Cary, USA). The p<0.05 was considered statistically significant. The authors compared the average variability between the groups and took the ratio of the between mean sum of squares (MSB) to the error (residual) of the mean sum of squares (MSE). That is, the F-statistic was calculated as F = MSB/MSE. The data for statistical analysis were reported as (F(between groups degree of freedom, residual error degree of freedom) = F-value, p-value). Any missing values for the study endpoints were not replaced, and the observed data was used for the endpoint analysis. The outcomes of participants who were randomized and received at least one intervention were carried out using the intention-to-treat (ITT) analysis. The results of the ITT analysis were compared with those of the per-protocol (PP) analysis to check whether the results were consistent or not.
Results
Disposition of study subjects
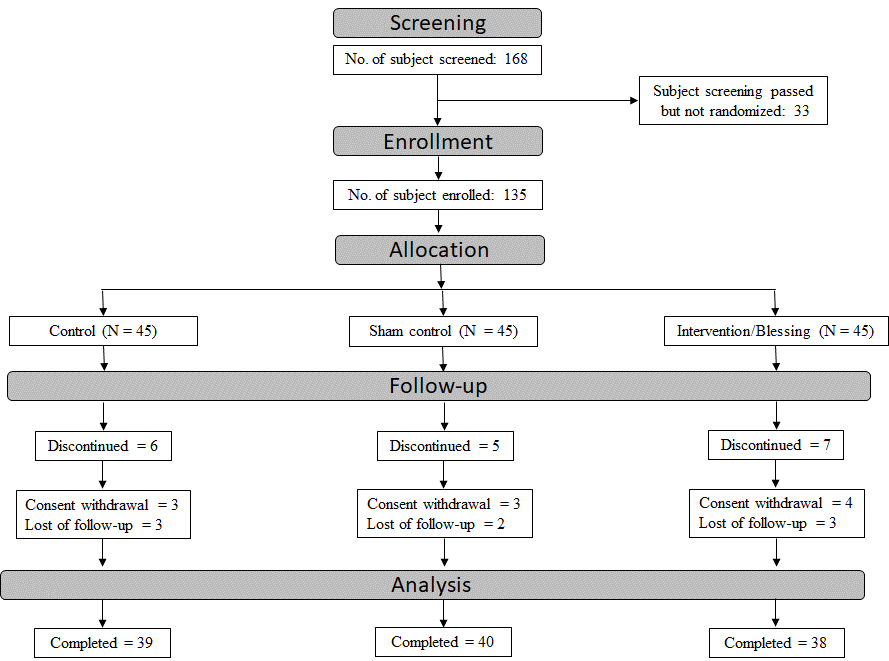
Briefly, 135 subjects were enrolled in the study out of the total 168 screened subjects, and 117 subjects completed the study. The subjects were assigned to the control group (39 subjects, including 18 males and 21 females), the sham control group (40 subjects, including 17 males and 23 females), or the remote biofield energy treatment group (38 subjects, including 21 males and 17 females). A total of 18 subjects were discontinued from the study during the study period. The reasons for discontinuation in the control and sham control groups were consent withdrawal by subjects (3 subjects each) and lost to follow-up (3 and 2 subjects, respectively). In the remote blessing/biofield energy treatment group, the reasons for discontinuation were consent withdrawal by subjects (4) and lost to follow-up (3 subjects).
Demographic and baseline characteristics
South Asian males and females aged between 20 and 55 years were included in the study. The mean age for subjects in the control group, sham control group, and blessing/biofield energy treatment group was 37.1 years, 37.1 years, and 37.3 years, respectively. The mean body mass index (BMI) for subjects in the control group, sham control group, and blessing energy treatment group was 26.11 kg/m2, 26.55 kg/m2, and 24.93 kg/m2, respectively. The percentage of male and female subjects in the control group, sham control group, and blessing/biofield energy treatment group was comparable, at 46.67%, 53.33%, and 55.56%, respectively. The majority of enrolled subjects were married, with rates ranging from 73.33% to 84.44%. Demographic characteristics such as body weight, age, sex, BMI, race, and smoking history did not show any significant differences, while height (p = 0.0428) and marital status (p = 0.0287) showed marginal differences across the study treatment groups, which did not affect the study outcomes (Table 1). The same demographic data have been reported in another manuscript for clarification and understanding of the results.
Assessment of Cognitive-motor Function Using NIH Toolbox®
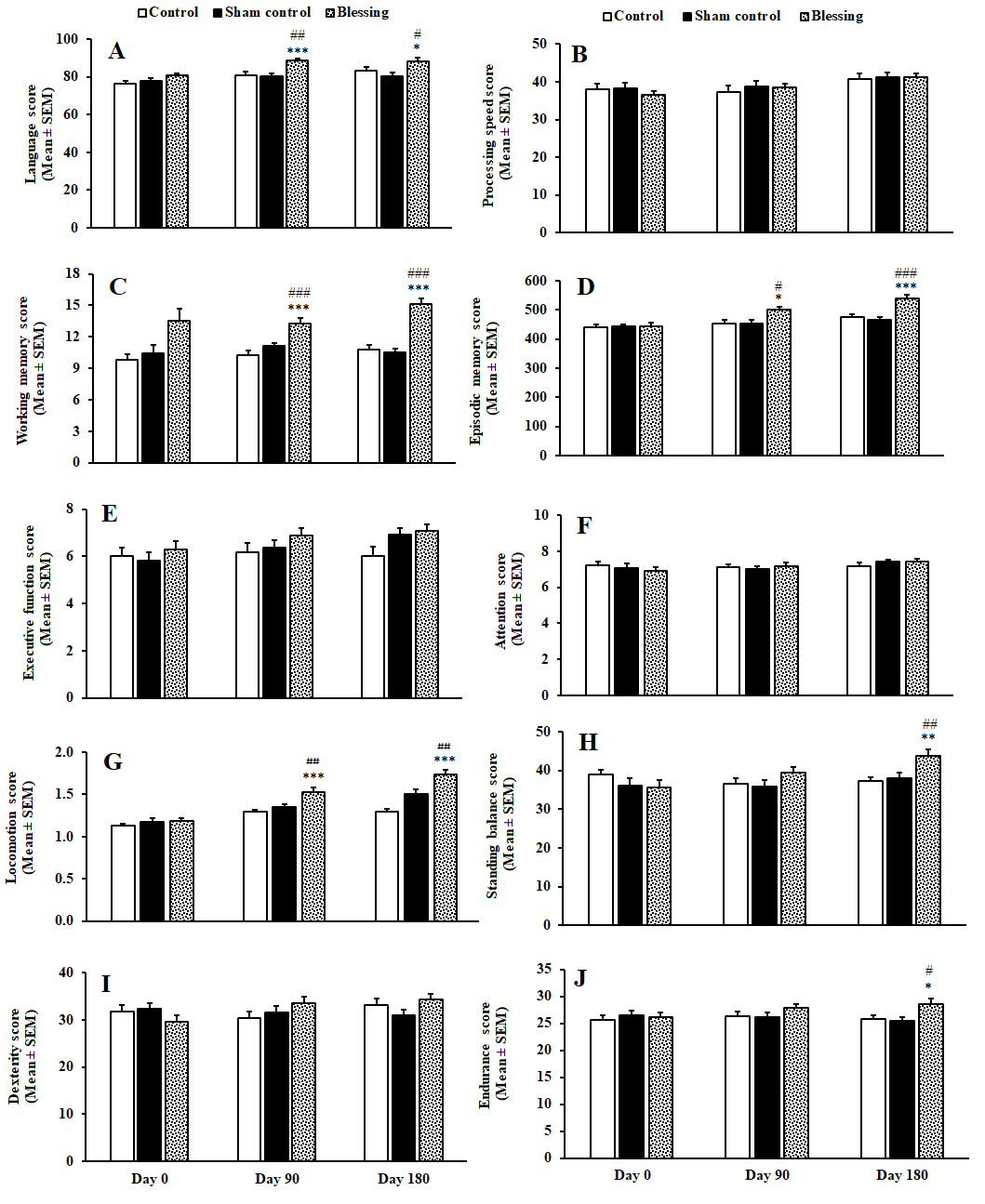
The comparison of parameters revealed no notable difference between the control and sham control groups. Figure 3 displayed the raw mean scores of the cognitive and motor function parameters before correction from the baseline values. However, a significant difference was observed in the language score, assessed by the NIH Toolbox® picture vocabulary test age 3+ v2.1, in the remote blessing/biofield energy treatment group at day 90 (F(2, 75) = 8.936, p <.001) and day 180 (F(2, 75) = 5.019, p = 0.020), compared to the control group. Moreover, the language score was considerably improved in the remote biofield energy treatment group at day 90 (F(2, 75) = 8.936, p = 0.002) and day 180 (F(2, 75) = 5.019, p = 0.022), compared to the sham control group. The Tukey’s post-hoc analysis revealed that the working memory function, assessed by the NIH Toolbox® list sorting working memory test age 7+ v2.1, was significantly improved in the distant blessing/ biofield energy treatment group at day 90 (F(2, 75) = 15.812, p <.001) and day 180 (F(2, 75) = 32.708, p <.001), compared to both control and sham control groups. The NIH Toolbox® picture sequence memory test age 8+ Form A v2.1 (episodic memory raw score) was found significant in the remote blessing treatment group assessed at day 90 (F(2, 75) = 5.251, p = 0.017) and day 180 (F(2, 74) = 18.521, p <.001) as compared to the control group. This score was further significantly improved in the remote biofield energy treatment group at day 90 (F(2, 75) = 5.251, p = 0.019) and day 180 (F(2, 74) = 18.521, p <.001) as compared to the sham control group.

Tukey’s post-hoc analysis revealed that the raw scores for processing speed, executive function, and attention, assessed using the NIH Toolbox® pattern comparison processing speed test, dimensional change card sort test, and flanker inhibitory control and attention test, respectively, did not show significant differences between the distant blessing/biofield energy treatment and control/sham control groups at both Day 90 and Day 180 (Figure 3A-3F). However, a statistically significant difference was observed in the motor domain measure of locomotion score (raw) using the NIH Toolbox® 4-meter walk gait speed test at Day 90 and Day 180, with the distant blessing/ biofield energy treatment group showing superior performance compared to the control group (F(2, 75) = 12.158, p <.001 and F(2, 75) = 28.614, p <.001, respectively). Additionally, this score was also statistically significant when compared to the sham control group at both time points (F(2, 75) = 12.158, p = 0.007 and F(2, 75) = 28.614, p = 0.002). Furthermore, Tukey’s post-hoc analysis revealed that the standing balance score (raw) assessed using the NIH Toolbox® standing balance test at Day 180 was significantly improved in the distant blessing/biofield energy intervention group compared to the control (F(2, 75) = 7.650, p = 0.003) and sham control (F(2, 75) = 7.650, p = 0.005) groups. However, there was only a marginal improvement in dexterity raw score, assessed using the NIH Toolbox® 9-hole pegboard dexterity test, in the distant blessing/biofield energy treatment group at both Day 90 and Day 180, and the data were non-significant. The endurance raw score by NIH Toolbox® 2-minute walk endurance test Age 3+ v2.0 was significantly improved in the distant blessing/biofield energy treatment group at day 180 as compared to the control (F(2, 75) = 5.095, p = 0.035) and sham control (F(2, 75) = 4.062, p = 0.012) groups (Figure 3G – 3J).
After applying the blessing/biofield energy intervention, the mean language score in the remote blessing/biofield energy treatment group was significantly improved from the baseline at day 90 (p = 0.0092) compared to the control group. Furthermore, significant improvements were seen in the distant blessing/ biofield energy treatment group at day 90 (p = 0.0031) and day 180 (p = 0.0056) compared to the sham control group in terms of working memory score. The working memory score in the distant blessing/ biofield energy treatment group was also significantly improved at day 90 (p = 0.0024) and day 180 (p <.0001) compared to the control group. Additionally, the NIH Toolbox® picture sequence memory test mean score (episodic memory) was significantly improved in the remote biofield energy treatment group at day 90 (p = 0.0025) and day 180 (p <.0001) compared to the control group. The episodic memory test score was further significantly improved at day 90 (p = 0.0024) and day 180 (p <.0001) in the distant blessing/ biofield energy treatment group compared to the sham control group. However, there was no significant difference in the processing speed and attention score in the distant blessing/biofield energy treatment group compared to the sham control or control groups (Table 2).
Besides, NIH Toolbox® 4-meter walk gait speed mean score (locomotion) was significantly improved at day 90 (p = 0.0009) and day 180 (p <.0001) in the distant blessing/ biofield energy treatment group compared to the control group; while this score also significantly improved at day 90 (p = 0.0104) and day 180 (p = 0.0006) in the distant blessing/ biofield energy treatment group compared to the sham control group. The NIH Toolbox® standing balance test score was significantly improved in the distant blessing/ biofield energy treatment group at day 180 as compared to the control (p = 0.0002) and sham control (p = 0.0020) groups. The score of NIH Toolbox® 9-hole pegboard dexterity test (dexterity) was significantly improved in the distant blessing/biofield energy treatment group at day 90 (p = 0.0185) compared to the control and at day 180 (p = 0.0085) compared to the sham control group. The NIH Toolbox® grip strength test score was significantly improved at day 90 (p = 0.0362) in the distant blessing/biofield energy treatment group than control group. Furthermore, NIH Toolbox® 2-minute walk endurance test score (endurance) was significantly improved in the distant blessing/ biofield energy treatment group at day 180 compared to the control (p = 0.0074) and sham control (p = 0.0007) group (Table 2). Based on the within-group analysis, a slight difference was observed in the mean score of cognition-motor function (between baseline and day 90/180) of some parameters. However, those differences were non-significant in the control or sham control group. Moreover, significant differences (p <.05 to p < .001) were found in the cognition-motor function mean score between baseline and distant blessing/ biofield energy treatment group at day 90/180 of parameters like standing balance, dexterity, episodic memory, executive function, language, locomotion, working memory, grip strength, and endurance.
Safety Assessment
No adverse effects (AEs) were reported during physical examination or during the entire study period. No clinically significant vital signs findings were observed during the study (Table 3). The hematological test results were within the normal range in all the groups (Table 4).
Discussion
Over the years, the topic of distant healing has been of great interest to researchers and clinicians, as it pertains to a phenomenon that is not yet fully understood. Distant healing intention (DHI) is a widely recognized form of complementary and alternative medicine (CAM) that involves remote biofield energy therapy (RBET).42 This particular form of therapy transcends traditional limitations of space and time, and is believed to positively impact the health and well-being of clients.17 In essence, DHI constitutes compassionate mental acts that are directed towards the improvement of another person’s health and well-being.43 Numerous studies have provided evidence of the successful healing effects of DHI. The primary therapies in this category include intercessory prayer, spiritual healing, aura healing, blessing, biofield energy healing, shamanic healing, non-local healing, therapeutic touch, quantum touch, qi gong, meditation, Johrei, and Reiki.19,44 The scientific evidence of quantum non-locality, which demonstrates the existence of an effect at a distance, and the evidence of quantum coherence in living systems, provide a foundation for potential explanations of DHI mechanisms.45–47
The present study’s findings strongly suggest that the exposure of distant blessing/ biofield energy therapy remotely has a positive impact on cognitive and motor functions, as measured by the NIH-TB cognition and motor functions battery. The study’s results are scientifically sound, robust, validated, and consistent, providing a solid foundation for drawing meaningful conclusions. This research presents the first comprehensive report on the effectiveness of distant blessing of significant improvements in cognitive and motor functions, as well as an assessment of neuropsychological properties. Our study indicates that exposure to blessing energy via remotely (distant healing) resulted in significant enhancements in cognitive performance, including language, working memory, and episodic memory, as well as motor performance, such as locomotion, standing balance, dexterity, and endurance, as assessed by the NIH Toolbox® cognitive and motor battery (Table 2). Shields et al. (2023) reported that the NIHTB-CB showed significant gains in almost all domains in individuals with intellectual disabilities, with individuals with Down syndrome exhibiting significant growth in early adulthood in two domains (working memory and attention/inhibitory control).48 In this trial, the distant blessing/biofield intervention group showed significant improvements in working memory function in cognitively deficient participants assessed by the NIH Toolbox® CB. Additionally, an expected pattern of memory and executive functioning improvements was observed in individuals with mild cognitive impairment (MCI).49 Of the NIHTB-M domains, deficits in endurance and balance were most prevalent. Physical function and mobility were successfully assessed in children with traumatic brain injury using the NIHTB-MB.50
The outcomes of the current study suggest a significant improvement in gait speed for the blessing intervention group compared to both the naïve control and sham control groups. Muscle endurance and cardiorespiratory functions are crucial components of physical fitness, performance, and overall health status. People with greater endurance are better equipped to handle daily tasks and high workloads. The current study’s results demonstrate a significant improvement in muscle endurance and cardiorespiratory functions. The NIH-Toolbox® findings in the cognitive domain indicate that four out of six parameters were statistically significant in the blessing treatment group, while in the motor domain, five out of five parameters were statistically significant compared to the control group. This study highlights the effectiveness of remote (distant) blessing/biofield energy therapy in improving neuropsychological functions, as assessed by the sophisticated NIH Toolbox® test battery.
The findings regarding the remote/distant-blessing energy therapy (R/D-BET) imply that it is feasible for individuals to interact remotely. This challenges the conventional notion of human interactions and communication within a specific location and time, which necessitates the presence of signals as proposed by classical physics. Additionally, it contradicts the notion of a strictly organic mind limited to the brain. Physics offers alternative theories that describe “non-local” forms of interaction that occur without the need for signals. One such theory is Entanglement theory, which suggests immediate physical correlations over large distances.20,21 Emerging theories propose that subjective mental activities, such as conscious awareness, can interact with reality in ways that the brain cannot.22 This suggests that R/D-BET is a non-local phenomenon.51 To gain a deeper understanding of how the expectations of participants and researchers may influence these effects, it is recommended that future studies be conducted by researchers from diverse backgrounds who possess expertise in non-local effects.
Possible mechanism of action
The precise mechanism of action for this healing therapy has not yet been completely clarified. There are various theories and beliefs regarding the efficacy of blessing/biofield energy therapy and spiritual healing. Recently published studies suggest that blessing/biofield energy therapies may have a spiritual aspect that functions at the quantum level, facilitated by the healer’s energy and thoughts. This can result in healing through instantaneous communication via quantum entanglement.52 Quantum entanglement enables instantaneous connection between system elements that are separated, which can be used for signaling across vast distances or in virtually.53 In this study, the authors speculate that the healer’s responses could be attributable to the quantum entanglement phenomenon. According to this study, it is suggested that human subjects receive remote biofield energies throughout their whole body. This information is then transmitted to the entire brain through the somatosensory system. The physiological hypothesis of this study is that biofield energy therapy activates different areas of the brain, resulting in enhanced cognitive and motor functions. This hypothesis assumes that blessing/biofield energy-based information is transmitted to the nervous (central and autonomic), immune, and endocrine systems. This provides a rationale for expecting that biofield energy therapy might influence the entire human body. This is believed to be the reason for the significant improvements in cognitive and motor function in adult subjects with perceived neuropsychological impairments. However, scientific research has not yet fully substantiated its explanatory power.
Strength of the study
Novelty and relevance: The study addresses the significant gap in the literature regarding the effectiveness of blessing/biofield energy healing therapies on cognitive and motor functions in adults, which is a novel and relevant area of scientific research.
Rigorous design: The use of a randomized, placebo-controlled, double-blind clinical trial design enhances the reliability and validity of the findings.
Comprehensive assessment: Utilizing the NIH Toolbox® for cognitive and motor function assessment, a well scientifically computerized software-based instrument, ensures a thorough and standardized evaluation of the outcomes.
Safety profile: The finding that there were no adverse effects and that physical vital signs and blood parameters remained normal is an important strength, underscoring the safety of the intervention.
Limitations of the study
Self-perceived impairments: The reliance on self-perceived neuropsychological impairments may introduce bias, as it is subjective and may not accurately reflect clinical diagnoses.
Virtual administration details: Although this study performed a blessing/biofield energy healing intervention virtually/distantly and achieved a significant outcome, the lack of detailed information on how the therapy was administered remotely makes it challenging to replicate the study.
Short follow-up period: The follow-up period of 180 days may be insufficient to fully capture the long-term effects of the intervention.
Sample size and single center: Although the sample size is reasonable, but a larger sample and multiple center trials would provide more robust data and enhance the generalizability of the findings.
Mechanism of action: Authors hypothesized that the findings might be due to the potential mechanism mentioned above. However, the exact mechanism of action is still unknown.
Limitations were also observed in the form of some ceiling effects on some tasks and floor effects, variable measurement sensitivity to cultural/socioeconomic factors.
Future research direction
Future research with larger sample sizes should provide greater clarity regarding the reliability and validity of the results within individuals. Further studies warranting investigation should include individuals with specific symptoms of various neurodegenerative disorders across all age groups, utilizing gold-standard testing methods. It is essential to explore the effects of distant blessing/biofield energy therapy on different populations and investigate a wider range of cognitive and motor function measures, as well as other domains from the NIH Toolbox®. Additionally, conducting mechanistic studies will contribute to a deeper understanding of the underlying biological processes involved in the therapeutic effects of biofield energy.
Conclusion
In conclusion, the study demonstrated that the remote (distant) blessing/biofield energy therapy resulted in significant improvements in cognitive and motor functions in adult subjects with perceived neuropsychological impairments in the treatment group as compared to the naïve control and sham control groups. These improvements ultimately led to enhanced physical functioning, overall health benefits, and quality of life in the subjects. Moreover, our findings suggest that the NIH Toolbox® is a reliable and valid tool for assessing neuro-psychological parameters in clinical populations.
Acknowledgments
The authors are grateful to Cliantha Research Ltd., Gujarat, India, for their assistance and support with the study. The authors also express gratitude to all participants and researchers who participated in this trial for their cooperation.
CRediT Author Contribution
A.B. and S.J. contributed to the study conception, design, planning, execution, monitoring, and data interpretation. S.M. and D.T. wrote the first draft of the manuscript. M.K.T. and S.J. contributed to the review and editing. All authors read and approved the final manuscript.
Competing Interests
Authors AB, MKT, and DT were employed by Trivedi Global, Inc. Authors SM and SJ were employed by Trivedi Science Research Laboratory Pvt. Ltd.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.