Introduction
Stroke is the second-leading cause of death and the third-leading cause of death and disability combined in the world, a situation that is consistent with the context in Thailand. The escalating healthcare burden of stroke in Thailand, with an estimated prevalence of 1.88% among adults over 45 years old, is primarily driven by the country’s transition to an aging society.1 Ischemic stroke treatment includes thrombolytic therapy, antiplatelet drugs, and mechanical thrombectomy. Additionally, it involves controlling blood pressure and cholesterol, adopting lifestyle changes, and undergoing rehabilitation therapy.2
Beyond the physical challenges, individuals who have experienced a stroke face an elevated risk of mental health issues such as depression, anxiety, and cognitive decline. Approximately 1 in 3 stroke patients may experience depression or anxiety within a year after the event, while 84% of stroke survivors encounter cognitive impairment within a 4-year period.3–5 The relationship between disability after stroke and depression has been studied. In a 2020 study conducted by Astuti et al., it was revealed that 62.5% of stroke patients experienced mild depressive episodes following the stroke, while 58.7% reported mild disabilities. Additionally, the study identified a correlation between the severity of depression and the extent of functional disability among post-stroke patients.6
Vascular function impairment constitutes a recognized risk of stroke. Dysfunctional blood vessels can precipitate the development of blood clots, atherosclerosis, and hypertension, collectively augmenting the propensity for stroke occurrence. The factors associated with vascular function include age, blood pressure, cholesterol levels, diabetes mellitus, obesity, medications, and physical activity. Various methods assess vascular function, including flow-mediated dilation (FMD) and brachial-ankle pulse wave velocity (baPWV). FMD gauges blood vessels’ capacity to expand in response to increased blood flow, reflecting endothelial function—a key cardiovascular health indicator influencing blood pressure regulation and vascular integrity.7,8 BaPWV measures the brachial-to-ankle artery pressure wave velocity, indicating artery stiffness; higher values suggest reduced elasticity, potentially signaling vascular aging and atherosclerosis. Both FMD and baPWV serve as clinical indicators for cardiovascular diseases, stroke, and congestive heart failure.9,10 Santos-García et al. also discovered that a decrease in FMD serves as an indicator for the occurrence of a new vascular event following a stroke.11
In the past decade, numerous studies have explored the link between vascular function and mental health, including mood and cognition. A prior systematic review and meta-analysis revealed an inverse relationship between depressed mood and endothelial function measured by FMD in both healthy individuals and cardiovascular disease patients.12 A 2016 systematic review also found that impaired FMD is associated with worse neuropsychological functioning, especially in executive function.13 In 2021, Moh et al. discovered that older individuals with type 2 diabetes exhibit elevated pulse wave velocity in correlation with depressive symptoms.14 A study in population-based by Nilsson et al. also found that cognitive function showed an inverse relationship with pulse wave velocity, displaying a nonlinear pattern.15 However, research on mental and vascular conditions in minor ischemic stroke or transient ischemic attack (TIA) patients, particularly in Thai patients, is limited.
This study aims to investigate the connections between vascular function (FMD and baPWV) and clinical characteristics (including age, gender, body weight, comorbidities, stroke classification, and duration of stroke), depression/anxiety, and cognitive function in these patients.
This study, approved by the Buriram Hospital Ethics Committee (IRB: BR0033.102.1/8), adhered to the Helsinki Declaration’s guidelines and obtained informed consent from all participants.
Materials and Methods
Participants
This research constituted a prospective cross-sectional investigation conducted among patients who had received treatment for minor ischemic stroke or TIA at the Neurology Outpatient Clinic of Buriram Hospital, a government regional hospital located in Buriram province, Thailand.
The inclusion criteria were as follows:
-
Aged between 40 and 70 years.
-
Diagnosed with a minor ischemic stroke (with a National Institutes of Health Stroke Scale score of 3 or lower) or TIA within a 5-year period.
The exclusion criteria were as follows:
-
History of atrial fibrillation.
-
History of anxiety or depressive disorders.
-
Denied participation in the study.
Data collection and measurements
Patients were provided with specific instructions before testing. They were advised to refrain from strenuous exercise for 24 hours, avoid caffeine and alcohol for 18 hours, and fast for 6 hours prior to their data collection appointment, which was scheduled between 8:00 AM and 9:00 AM at the hospital. Patients were also advised to wear comfortable, lightweight clothing and remove any metal items. The testing sessions, which included completing a questionnaire, assessing body composition, measuring baPWV, and evaluating brachial FMD, occurred between 8:00 AM and 11:00 AM in a controlled environment maintained at approximately 23–25 degrees Celsius.
Questionnaire, body composition, and medical records
The Hospital Anxiety and Depression Scale (HADS) questionnaire, comprising HADS depression (HADS-D) and HADS anxiety subscales (HADS-A), was employed to assess anxiety and depression.16 Cognitive function was measured using the mini-mental state examination (MMSE) and Montreal cognitive assessment (MoCA).17 Data from the HADS, MoCA, and MMSE were gathered by a psychiatrist. We employed an Omron HBF375 body composition analyzer (Omron Healthcare Europe B. V., Hoofddorp, Netherlands) to assess body composition, including weight, body fat percentage, and basal metabolic rate. Clinical data, including low-density lipoprotein (LDL) and glycated hemoglobin (HbA1c) levels measured within the last 4 weeks, along with other clinical characteristics, were extracted from medical records.
Brachial flow-mediated dilation (FMD)
The characteristics of the brachial artery were assessed using ultrasound equipment (Vividi, GE Healthcare, Cardiovascular Ultrasound System; GE Medical Systems, Tirat Carmel, Israel). All participants were instructed to remain in a supine position for 20 minutes before the measurement, and a blood pressure cuff was placed around the right forearm for the duration of the measurements. The brachial artery’s features were longitudinally recorded from the antecubital fossa at three time points: 1 minute at baseline, 5 minutes during occlusion, and 3 minutes during deflation.18,19 During the occlusion phase, the cuff was inflated to a pressure 50 mmHg above the systolic blood pressure.7 To minimize potential investigator bias in image analysis, a computer-based analysis program (Brachial Analyzer, Medical Imaging Applications, Coralville, IA, USA) was employed to analyze changes in vascular diameter. FMD was determined using the formula FMD = (d2 - d1) x 100/d1, where d1 represents the average brachial artery diameter at baseline and d2 denotes the average brachial artery diameter after occlusion.20
Brachial-ankle pulse wave velocity (baPWV)
The baPWV was assessed using a non-invasive vascular screening device (OMRON; Colin VP-1000 plus, Kyoto, Japan). Participants were positioned in a supine posture and equipped with electrocardiogram and phonocardiogram electrodes, placed on the left edge of the sternum or around the second intercostal space. Subsequently, cuffs with electrocardiography electrodes were wrapped around the wrists and brachium, as well as the ankles. These cuffs were then connected to a plethysmographic sensor for volume pulse form analysis and an oscillometric pressure sensor to determine blood pressure. Finally, the pulse volume waveforms of the brachial and ankle were recorded over approximately 10 seconds of cardiac cycles, and the average baPWV value was computed from both the right and left sides.
Statistical analysis
Data analysis was conducted using IBM SPSS Statistics version 19 (IBM Corp., Armonk, NY, USA). Descriptive statistics, including counts, percentages, means, and standard deviations (SD), summarized participants’ general information. Linear regression analysis was used to explore factors linked to continuous variables, such as FMD and baPWV. Statistical significance was established at P < 0.05.
Results
The clinical characteristics of the 23 participants included in the current study are shown in Table 1. The group consisted of 14 males (60.9%) with a mean age (SD) of 58.9 (7.57) years. The average body weight was 72.8 kg, with a mean body fat percentage of 32.0%. Common comorbidities included hypertension (82.6%) and diabetes mellitus (60.9%). The Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification revealed that 30.4% had large artery atherosclerosis, while 69.6% had small vessel occlusion. Cognitive function was assessed using MMSE and MoCA, with mean scores of 23.9 and 19.0, respectively. Anxiety and depression levels were measured using HADS, with mean scores of 4.5 for anxiety and 3.5 for depression. Vascular function parameters included a mean baPWV of 1,716.9 cm/s and a mean FMD of 5.0%.
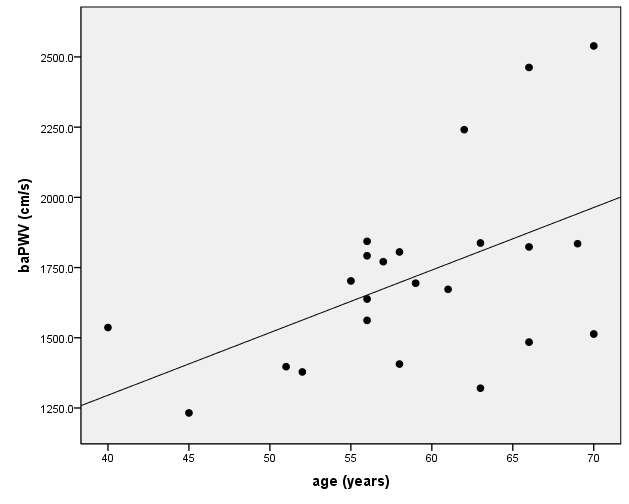
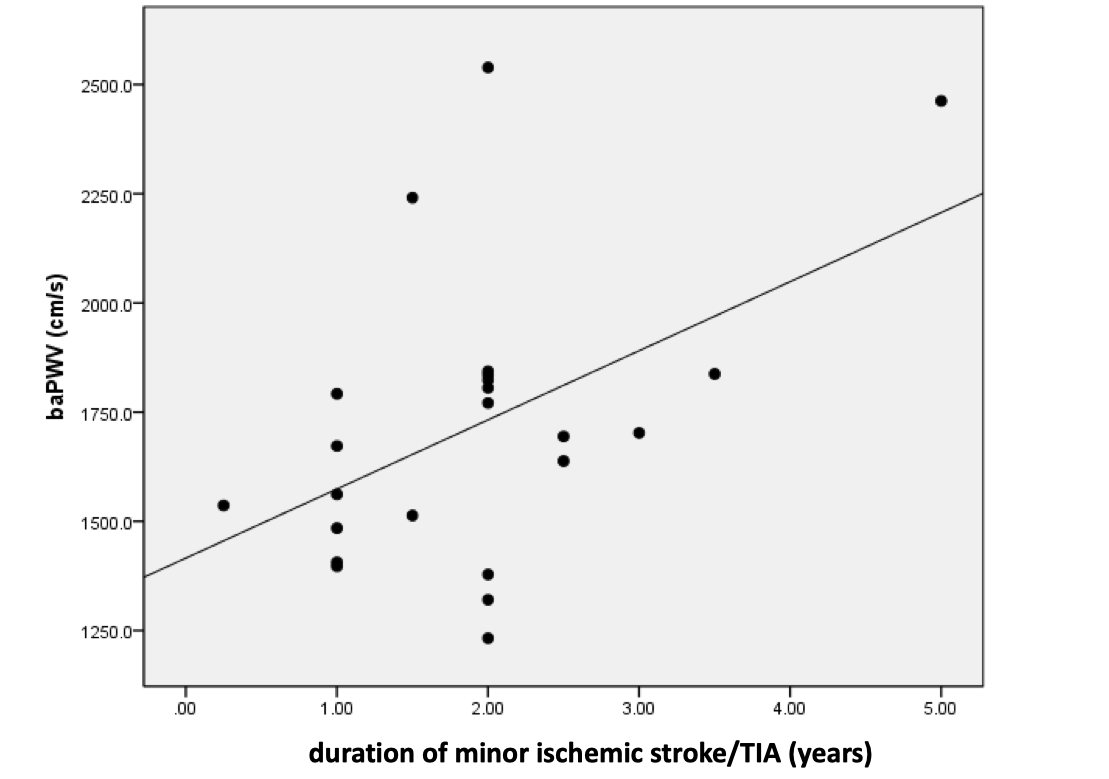
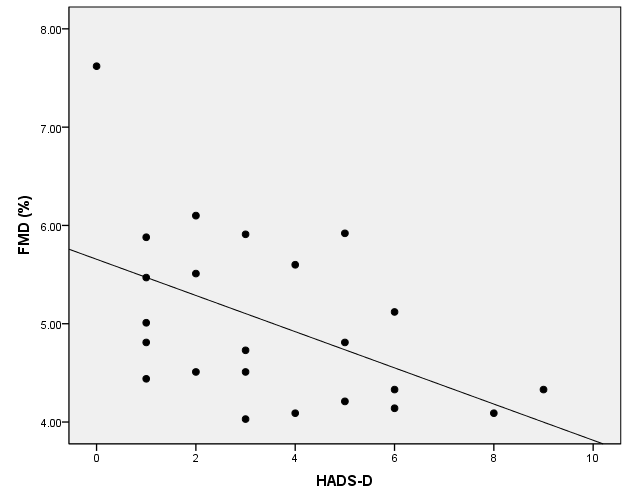
Table 2, Figure 1, Figure 2, and Figure 3 illustrate the relationships between clinical characteristics, mental health, and vascular function in minor ischemic stroke or TIA patients. A significant positive relationship exists between age and baPWV (β = 0.51, p = 0.014), suggesting that as age increases, baPWV tends to increase. Additionally, there is a significant positive relationship between the duration of minor ischemic stroke or TIA and baPWV (β = 0.48, p = 0.022), implying that a longer duration of stroke or TIA is associated with higher baPWV. Moreover, a significant negative relationship is observed between HADS-D score and FMD (β = -0.50, p = 0.015), indicating that higher depression scores are linked to lower FMD. Furthermore, a marginally significant negative relationship is found between MMSE score and baPWV (β = -0.38, p = 0.073), suggesting that lower MMSE scores (indicative of cognitive impairment) are associated with higher baPWV. Lastly, a marginally significant positive relationship is found between HbA1c and baPWV (β = 0.38, p = 0.073). Notably, there were no statistically significant associations between vascular function (FMD or baPWV) and other clinical characteristics, including MoCA, HADS-A, body weight, body fat, basal metabolic rate, body mass index, LDL, systolic blood pressure, diastolic blood pressure, and mean arterial blood pressure.



Discussions
The present study investigated factors related to vascular function in minor ischemic stroke or TIA patients, and the evaluation can be divided into three parts. The first part of the study centered on clinical characteristics. We discovered a connection between age and the duration of minor ischemic stroke or TIA, and baPWV. This correlation could be attributed to the influence of aging on arterial stiffness, possibly due to endothelial dysfunction. It’s plausible that more advanced age or a longer duration of stroke or TIA could contribute to increased arterial stiffness.21
The second part of our study focused on cognitive function. We found a marginally significant negative relationship between MMSE score and baPWV (β = -0.38, p = 0.073), indicating that lower MMSE scores (indicative of cognitive impairment) are associated with higher baPWV. Our findings align with previous studies that have demonstrated a modest association between high arterial stiffness, as measured by pulse wave velocity, and cognitive decline and impairment.15,22 This association might be explained by: 1) High pulse pressures may alter cerebral blood vessel structure, hindering the transport of nutrients to the brain and the removal of toxic byproducts. 2) White matter damage: Arterial stiffness contributes to the formation of white matter lesions in the brain, disrupting communication between brain regions and affecting cognitive processes. 3) Arterial stiffness serves as an independent predictor for cardiovascular events and risk factors, which subsequently influence cognitive decline.22
Depression and anxiety were discussed in the third part. A higher level of depression may impair FMD in stroke or TIA patients, as shown by the negative correlation between FMD and HADS-D in our study. We posit four reasons for the connection between depressive symptoms and impaired FMD in minor ischemic stroke or TIA patients (1) Inflammation: Depression is linked to chronic low-grade inflammation, which negatively affects endothelial function including blood vessel dilation.23,24 (2) Oxidative stress: Depression elevates oxidative stress, and this increase in oxidative stress leads to damage in blood vessel walls, resulting in FMD impairment.25 (3) Autonomic nervous system imbalance: Depression impairs autonomic nervous system regulation, causing abnormal blood vessel responses, which might lead to impaired FMD.26 (4) Physical inactivity: Depression frequently results in reduced physical activity, contributing to endothelial dysfunction. Considering the association demonstrated in a previous study between impairment of FMD and the occurrence of a new-onset vascular event following a stroke, our findings emphasize the importance for physicians to pay attention to stroke patients experiencing significant depression.11
Narita et al. discovered a significant inverse relationship between anxiety and FMD in elderly individuals, a connection not found in younger subjects. This implies that anxiety might serve as a predisposing factor for cardiovascular damage, potentially contributing to the development of atherosclerotic lesions over time.27 The mechanisms behind anxiety-induced vascular impairment can be elucidated through the following pathways. (1) Activation of sympathetic activity: Anxiety triggers the release of stress hormones such as adrenaline and cortisol, heightening sympathetic activity. This increased activity may result in vasoconstriction and elevated heart rate, thus contributing to vascular dysfunction.28 (2) Inflammation and oxidative stress: Chronic anxiety is linked to systemic inflammation and oxidative stress. Elevated levels of pro-inflammatory cytokines and reactive oxygen species can harm the endothelial cells lining blood vessels, impairing their function and contributing to atherosclerosis.29 (3) Dysregulation of the Hypothalamic-Pituitary-Adrenal (HPA) Axis: Anxiety can disrupt the HPA axis, leading to excessive cortisol production. Prolonged exposure to high cortisol levels may disrupt vascular homeostasis and impair endothelial function.30 (4) Behavioral risk factors: Individuals experiencing anxiety may engage in unhealthy behaviors such as smoking, poor dietary choices, physical inactivity, and substance abuse, all recognized as risk factors for vascular impairment. These behaviors can exacerbate vascular dysfunction and heighten the likelihood of cerebrovascular diseases.31–33 In the present study, we did not observe a significant association between anxiety, as measured by HADS-A, and vascular function. However, we believe that such an association might emerge if we increase the number of participants and/or utilize another or multiple tests for measuring anxiety.
This study has several limitations. Firstly, it had a limited sample size; future research should consider a larger sample for more robust results. Secondly, future studies could benefit from assessing parameters like nitrite/nitrate and endothelin-1, as these were not measured in our research, potentially providing insights into changes in blood chemistry. Lastly, our study did not evaluate smooth-muscle function, which could offer additional insights into the observed alterations in FMD.
Conclusions
FMD exhibits a connection with depressive symptoms, while baPWV demonstrates associations with both age and the duration of stroke or transient ischemic attack among patients suffering from these conditions. As a result, understanding the interplay among these factors could prove valuable for physicians in monitoring and predicting disease progression.
Author Contributions
Conceptualization, Witid Mitranun and Witoon Mitarnun; Methodology, Witid Mitranun and Witoon Mitarnun; Resources, Witid Mitranun and Witoon Mitarnun; Data Curation, Witid Mitranun and Witoon Mitarnun; Writing—Original Draft Preparation, Witid Mitranun, Witoon Mitarnun, Prasit Peepathum, Amorntheap Wandee, Wenika Mitarnun, Wilasinee Pangwong, and Tanormsak Senakham; Writing—Review and Editing, Witid Mitranun, Witoon Mitarnun, Prasit Peepathum, Amorntheap Wandee, Wenika Mitarnun, Wilasinee Pangwong, and Tanormsak Senakham. All authors have read and agreed to the published version of the manuscript.
Conflict of Interest Statement
The authors declare that there are no potential conflicts of interest regarding the research, authorship, or publication of this manuscript.
Acknowledgment
This work was supported by (i)Srinakharinwirot University (SWU), (ii)Thailand Science Research and Innovation (TSRI), and (iii)National Science Research and Innovation Fund (NSRF) (Fundamental Fund: Grant no.006/2565).
Data sharing statement
We declare that the data supporting the findings of this study are available.