INTRODUCTION
Body dysmorphic disorder, BDD, is characterized, as reported by the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) by excessive preoccupation with at least 1 perceived defect in physical appearance that is not evident or almost imperceptible by other people. This preoccupation with physical appearance must cause clinically significant distress or impairment in social, work, and school activities. BDD is characterized by the presence of at least 1 repetitive behavior that is enacted as a consequence of obsessive thinking.1 Although it was first described in 1891 by E. Morselli, body dysmorphic disorder was not included until 2018 in ICD-11 as an independent diagnostic category among “obsessive-compulsive or related disorders.” Even today, it is often underdiagnosed, especially among adolescents, who are the target group most affected by the disorder.
A model termed “LIBET” has schematized in simple steps the life history of the patient with body dysmorphism disorder, describing: a cold living environment with a critical and demanding context; a high importance associated with body image and beauty; a culture predominantly based on individuality; the presence of intolerable mental schemas; and the tight belief in being ugly. This leads to: the belief that one is rejected; the presence of pathological life plans characterized by avoidance and compulsion to control imperfections, perceived through the succession of actions aimed at eliminating perceived flaws and the emergence of a good self-image.2
Several studies3–5have in fact identified that the onset of the disorder is more frequent before the age of 18 and rare after the age of 40, showing that onset in adolescence does not determine a greater severity in the symptomatology of the disorder. The nidation of its development during this period is closely related to the characteristics of that phase of life during which the body and mind undergo strong changes that lead, very often, to finding oneself “children locked in the body of an adult” or vice versa.
The absence of awareness of body dysmorphism disorder among adolescents, and the diagnosis in adulthood, appears to be a consequence of the inherent characteristics of that stage, in which discomfort toward one’s body, or a part of it, appears to be the norm, which induces less demand for help. In fact, most young people normally worry about their physical appearance, which induces underestimation of symptomatology and diagnostic difficulty. Our research objective was to observe which therapy was most effective in treating and monitoring the symptomatology of BDD disorder.
Our diagnostic hypothesis was that cognitive behavioral therapy was the elite therapy for the treatment of the disorder. Cognitive- Behaviour Therapy (CBT) was first defined in the 1960s by Aaron Beck and Albert Ellis (Beck 1967, Ellis 1962), who defined that “pathology is the result of dysfunctional thoughts, patterns and processes.” It has as its main goal to change patients’ distorted beliefs by modifying dysfunctional thoughts and behaviors until the removal of the symptom causing extreme distress to the subject is achieved. It is based on the thought that events do not form the behavioral, emotional or psychological problems, but these are influenced by the cognitive constructs already present in the individual.
In fact, CBT, has as its primary goal to identify the individual’s dysfunctional thoughts and reasoning patterns in order to replace them with functional beliefs. Moreover, among CBT therapies, the therapy that has had positive impacts on the treatment of the disorder in recent years has been CBT-NET. Since this is an entirely online treatment, which does not require much effort on the part of patients, it is very easy to use. The treatment consists of the ability to receive or send questions/answers between therapist and patient, with unlimited availability in doing so. The therapist’s main task is to guide and help the patient in treatment by answering questions and providing support.
BDD-NET appears to be effective, as it is pocket-friendly and accessible at any time of the day responding directly to the patient’s needs.
The review we conducted confirmed our original hypothesis, showing that cognitive behavioral and related therapy appears to be the most effective of the therapies reviewed, especially when combined with drug therapy.
MATERIALS AND METHODS
Search strategy.
The systematic review was conducted according to the PRISMA 2020 guidelines for systematic reviews of the PRISMA Group. From February 2022 until October 2022, we used databases such as PubMed, MedLine, and PsycInfo to identify relevant studies, using specific search terms: “body dysmorphic disorder,” “body dysmorphic disorder treatment,” “body dysmorphic disorder and plastic surgery,” and “body dysmorphic disorder and CBT* OR BDD- NET.” The electronic search was expanded through a manual search of the reference lists of included articles to identify additional sources.
Eligibility criteria
We included any article without language restriction but from a time period between 2015 and 2022 meeting the following criteria: (1) Participants: patients with body dysmorphic disorder. (2) Intervention: any topic that related to body dysmorphism disorder and the most common and functional strategies for its treatment. (3) Comparison: any intervention that is used for the treatment of body dysmorphism disorder, such as: CBT; BDD-NET; Psychoeducation; Drug therapy; Cosmetic therapy. (4) Results: we considered the results that delved into BDD in its relevant aspects, in the most discussed and used psychotherapeutic interventions and cosmetic treatments in the time period described in the eligibility criterion.
Data extraction
We extracted the data using parameters in particular: characteristics of the samples and the completed study, when the study was done, intervention used, keywords of the study, duration and frequency of treatments and the study, presence of follow-up, results and objectives of the study.
Risk assessment of bias
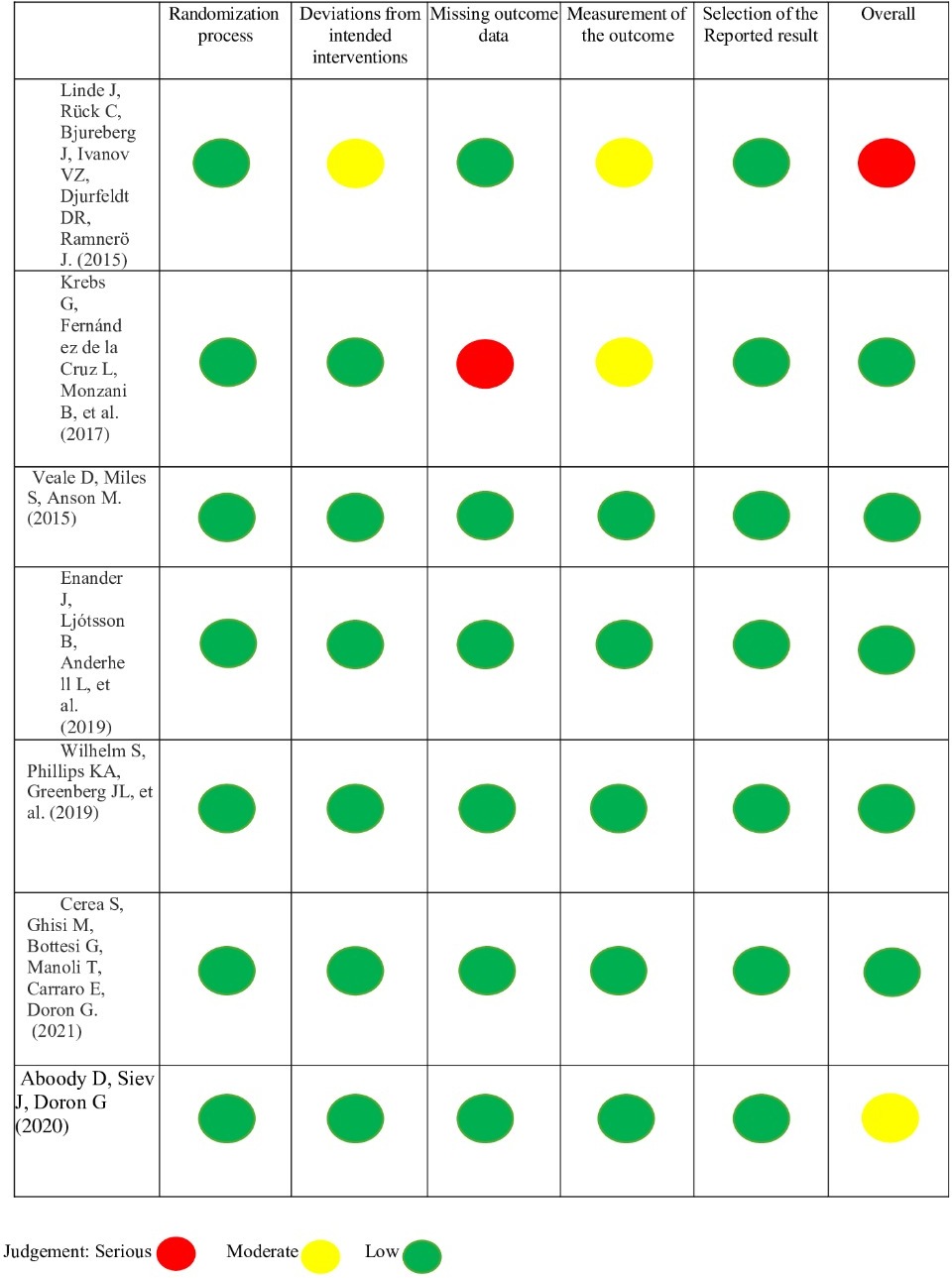
The risk of bias for included studies was assessed with the Cochrane risk-of-bias tool for randomized trials, version 2 (RoB 2) by Sterne et al.
RESULTS
Characteristics of included studies
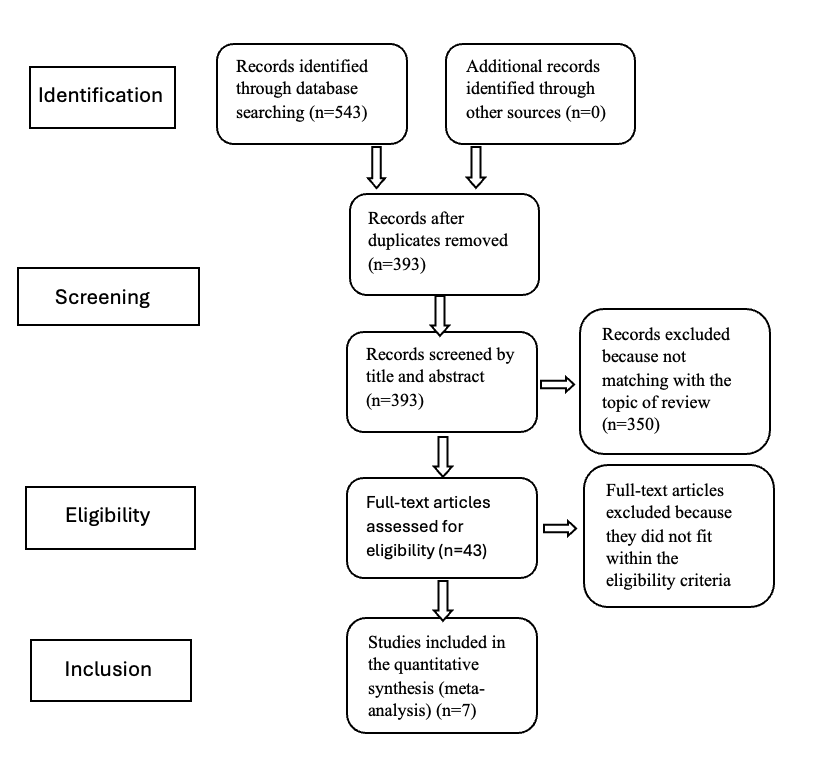
The database search identified a total of 543 articles. We read the articles in their entirety and excluded 150 duplicates, managing to identify 393 articles of interest to the aim of our systematic review. More than 350 articles were excluded because they did not correspond to the intent of our systematic review. Forty-three articles were studied for suitability, among which seven (n = 7) of these were chosen and included in the review because they fit the proposed objective. The studies included in our systematic review have been summarized in Figure 1, and the data extraction of these studies can be viewed in Table 1. To conclude, in Figure 2, we have included the risk assessment of bias for the included studies.


Acceptance-Based Exposure Therapy for Body Dysmorphic Disorder: A Pilot Study.6
This pilot study aimed primarily to examine the feasibility of acceptance-based exposure therapy in 21 patients for in BDD. The treatment consisted of a total of 12 weekly group sessions of 180 minutes each and weekly individual sessions of 60 minutes starting from the third week of treatment. Of the 21 patients who participated in at least one treatment session, only 19 completed treatment. The results suggest that acceptance-based exposure therapy is feasible to implement and appears to be an effective treatment for this disorder. follow-up data showed that patients maintained their results for at least 6 months after completing treatment. However, the present study contains a number of limitations: the study had a small sample size and lacked a control group.
Long-Term Outcomes of Cognitive-Behavioral Therapy for Adolescent Body Dysmorphic Disorder.7
This study primarily aimed to follow a group of adolescents who had originally participated in a randomized, controlled trial of CBT for BDD to determine whether treatment gains were maintained. The RCT8 included 30 adolescents with BDD who were randomized to receive 14 sessions of CBT for 4 months or to a control condition involving written psychoeducational materials and weekly telephone monitoring for 4 months.
CBT was found to be associated with a significant reduction in symptoms of bipolar disorder, and improvements were maintained until the 12-month follow-up. There are limitations in this study: small sample; naturalistic follow-up of an RCT; absence of control group; numerous deviations from protocol; recruitment of adolescents with severe BDD symptoms.
Long-Term Outcome of Cognitive Behavior Therapy for Body Dysmorphic Disorder: A Naturalistic Case Series of 1 to 4 Years After a Controlled Trial.9
The present study is a follow-up report by Veale, Anson et al. (2014)10 who conducted an RCT to determine whether CBT had greater efficacy than anxiety management (AM) in BDD. This is the first study to examine a naturalistic outcome of CBT for BDD of a cohort of participants in the long term after 1-4 years.
Forty-six participants were randomly assigned to CBT or AM. The primary endpoint was at 12 weeks, and the CBT group, unlike the AM group, had four weekly sessions Both groups completed the measures at the 1-month follow-up. At 12 weeks, CBT was significantly superior to AM on the BDD-YBOCS. The main limitations of the study are the lack of a comparison condition and a retrospective design.
Long-term outcome of therapist-guided internet-based cognitive behavioral therapy for body dysmorphic disorder (BDD-NET): a naturalistic 2-year follow-up after a randomized controlled trial.11
This study is the first to explore the long-term outcomes of a new Internet-based, therapist-driven program designed to increase access to cognitive-behavioral therapy for patients with body dysmorphic disorder. In one RCT,12 BDD-NET was associated with significant improvements in BDD symptom severity, depression, and other short-term secondary outcomes.
88 participants from the original sample of 94 received Internet-based CBT and were included in long-term follow-up. BDD-NET is effective in the long term and has the potential to increase access to CBT for people with BDD. There are limitations in this study: no control group and participants had a fair amount of insight such that the results cannot be generalized to all people with BDD.
Efficacy and Posttreatment Effects of Therapist Delivered Cognitive Behavioral Therapy vs Supportive Psychotherapy for Adults With Body Dysmorphic Disorder: A Randomized Clinical Trial.13
This randomized clinical trial’s main objective was to test whether CBT was superior to supportive psychotherapy for treating BDD symptoms and to test the maintenance of results over time. Patients were recruited in a hospital setting and were divided into 61 for CBT and 59 for supportive psychotherapy. Both treatments consisted of 22 individual 60-minute sessions for 24 weeks. The results show that BDD symptoms decreased statistically significantly more in CBT-BDD than in supportive psychotherapy at the end of treatment. Limitations of the study were: predominantly female and well-educated sample and lack of random assignment to therapists.
Cognitive Behavioral Training Using a Mobile Application Reduces Body Image-Related Symptoms in High Risk Female University Students: Randomized Controlled Study.14
This randomized, controlled trial primarily aimed to evaluate the effectiveness of a mobile application, based on cognitive behavioral principles, to reduce body dissatisfaction and BDD symptoms in female college students considered to be at high risk of developing body image disorders. Thus, 50 college students were divided into two groups: the first group started treatment with the App first and for 16 days while the second group waited 16 days before starting to use the App. Results show that exercising 3 minutes a day for 16 consecutive days with the GGBI App brought moderate reductions in some forms of body dissatisfaction, including BDD symptoms. Limitations include small sample and recruitment occurred based on smartphone operating systems.
Building resilience to body image triggers using brief cognitive training on a mobile application: A randomized controlled trial.15
This randomized controlled trial recruited a nonclinical sample of 90 women to subject them to using the mobile app for 4 minutes of exercise per day for about two weeks. The presence of a control group confirmed that those who used the app (GGBI) had a potential reduction in BDD symptoms, and the results were maintained at the one-month follow-up.
This randomized controlled trial recruited a nonclinical sample of 90 women to subject them to using the mobile app for 4 minutes of exercise per day for about two weeks. The presence of a control group confirmed that those who used the app had a potential reduction in BDD symptoms, and the results were maintained at the one-month follow-up. Limitations concern: the participants were all female college students, and the control group was not active but on a waiting list.
DISCUSSION
The research conducted through a systematic literature review allowed us to observe that the most effective psychotherapy therapy in treating and monitoring the symptoms of body dysmorphic disorder is cognitive behavioral therapy (CBT). This research result correlates positively with our original hypothesis. Furthermore, it turns out that the preferred treatment of patients is plastic surgery, which induces a spiral of interventions to end a defect that does not really exist but is a result of the disorder itself.
Body dysmorphic disorder (BDD), still underdiagnosed especially among young adolescents, is a disabling disorder, affecting an individual’s quality of life and psycho-social functioning. The body (which enables the construction of identity) is the central and most important issue for the BDD patient. Human beings are concerned with how others see them; this affects their self-esteem, which is “like a product that arises from interactions with others, which is created over the course of life as a reflected evaluation of what other people think of i us.” (Mead & Cooley, n.d)
Several studies have shown that BDD is associated with low self-esteem and how it is negatively correlated with symptom severity.16
The patient turns out to be distressed and threatened in his or her “ideal image,” so he or she begins to enact desperate behaviors to restore this image so as to bring it closer and closer to what turns out to be ideal for him or her.
Often insight in people with BDD is absent or poor (individuals with BDD are mostly or completely convinced that they look abnormal, ugly or deformed), such individuals in fact, are unwilling to engage in mental health treatment preferring cosmetic treatment. For example, 47% of young patients with BDD desire cosmetic treatment with about 33% actually receiving, actually, these desired interventions.17
Most people with BDD believe that their problem is physical rather than psychological and therefore seek refuge in plastic surgery. BDD rates of 12.3% have been reported in general cosmetic surgery settings, 20.1% in patients undergoing rhinoplasty, 5.2% in cosmetic dentistry, and 9.2% in cosmetic dermatology.18
Precisely because the areas most affected in individuals with BDD are skin, or at any rate parts of the face, the physicians most frequently consulted by patients are dermatologists. The latter are frequently contacted as an attempt to resolve certain issues, which arise from the compulsions of patients with BDD, among which we find excoriation disorder and trichotillomania.
Some patients with BDD have reported spending more than eight hours a day trying by various means (hands, razor blades, tweezers, needles) to eliminate their defects, which almost always results in the emergence of lesions and seeking surgery.19
Although such patients constantly seek, to end their discomfort through cosmetic surgery, one research study highlights how some people with BDD experience, after surgery, a brief relief that ceases after a circumscribed period of time. This fuels in them the desire to undergo surgery again for the same or another physical defect.20
In fact, very often individuals with BDD who undergo cosmetic surgery or dermatological treatment feel, at the end of their journey, that not only was the surgical treatment ineffective, but that the latter even worsened the situation leading them to physically threaten those who operated on them.21
For this reason, recognition of body dysmorphic disorder before implementing cosmetic treatment is considered of paramount importance in order to eliminate possible consequences and as such treatment does not lead to greater well-being.
Despite such data showing the ineffectiveness of cosmetic treatment in treating the symptoms of BDD, a recent study affirms the importance of sophisticated decision making that focuses on the severity of the disorder and the general level of functioning of patients, using refined tools for suitability for cosmetic procedures.22
The therapy with the greatest effectiveness is cognitive-behavioral therapy, which induces remission of symptoms. A study by Rosen and Reiter (n.d.), found the extent to which cognitive-behavioral therapy can improve the symptoms of BDD to increase the patient’s self-esteem. Increasing self-esteem, for example, could be seen as a prevention of BDD.23
The propensity of the patient with BDD to seek surgical intervention may lead to lack of good motivation if psychotherapeutic treatment is referred. The treatment most often turned to for the treatment of body dysmorphism disorder is cognitive behavioral therapy. Like any other treatment, we know that for therapy to be functional and effective, building a good therapeutic alliance is important. In this field, this goal can be difficult to accomplish due to lack of insight (as evidenced by the various studies previously reviewed). In order for the therapeutic work, which the patient must complete, to lead to real improvements, the force separating the ideal self from the real self must be reduced to the minimum possible.
Patients with BDD, fail to have a clear representation of their image, but more importantly, they do not possess the awareness that in addition to the perceived flaws there are strengths that they have failed to grasp.
Through self-awareness and increased self-esteem, the patient may be able to realize the disorder and form a perception that is functional in nature. The main goal is, based on the process that characterizes the patient with the disorder, a modulation of selective attention that is directed to the smallest details and an improvement in the ability to synthesize. We have already expressed the importance of self-esteem, which is found to be significantly low in patients with BDD, so it is of central importance that the patient through treatment decenters from the ideal (unattainable) self to focus on the strengths of the real self in order to raise self-esteem.
The study of different psychotherapeutic interventions was important in confirming our original question, namely, to identify the most effective treatment for the symptoms of body dysmorphic disorder.
CBT for treating patients with BDD was highlighted within a study where it explained that cognitive behavioral therapy for BDD typically begins with psychoeducation, during which the therapist explains and identifies the cognitive behavioral model of BDD. In addition, CBT usually includes techniques such as self-monitoring of automatic negative thoughts and behaviors along with exposure and prevention of response as well as relapse.24
A difficulty emerges in patients with BDD in initiating CBT therapy, both due to economic issues and patients’ lack of tendency to seek psychological treatment. In addition, poor patient insight is associated with poorer CBT response.
One of the most effective and innovative CBT therapies to date is BDD-NET, which seems to be useful, as it takes advantage of one of the conditions we find ourselves experiencing in recent decades, namely, the use of the Internet. It seems to be effective both in terms of cost but also in terms of benefits.
The BDD-NET is an online platform, which allows patients not to have direct physical interviews with the therapist, a plus point for patients with BDD who experience feelings of guilt and shame about their condition. Patients are required to respond to eight modules, with timelines that suit their needs, covering different topics such as: - cognitive restructuring; - psychoeducation; - values-based behavior modification; - exposure and response prevention; - relapse prevention; - conceptualization of BDD; and - difficulties encountered during treatment. In the study, patients were observed and evaluated by telephone before, during and at the end of treatment (immediately - 1 year later - 2 years later). All participants added additional treatment to BDD-NET: psychological or pharmacological. The results confirmed that BDD-NET brought significant improvement in symptoms: 40% of participants maintained improvement after one year, 29% had a slow response to treatment, and 10% of subjects, who had a good response to treatment, manifested a relapse at one year of the end of it. Depressive symptoms were found to have decreased at one year after treatment, while global functioning was significantly improved at two years after treatment. One of the participants had undergone plastic surgery twice two years after the end of treatment. The results of this study confirm the long-term effectiveness of CBT on improving BDD symptoms.25
CONCLUSION
Our main research objective was also to identify the most effective treatment for remission of symptoms associated with BDD.
The data from the existing scientific literature in the field highlight CBT as the most effective and efficient therapy, especially in combination with pharmacological treatment.
In addition, cognitive behavioral therapy utilized through Internet platforms through the use of specific applications, including BDD-NET, has revealed significant results for the remission of BDD symptoms.
Furthermore, it has emerged that only in recent years, with the increase in the number of individuals requiring surgical treatment, has the importance given to the disorder ponderously increased.
Nevertheless, we believe that it is important to conduct further long-term studies and on a larger sample, in order to obtain generalizable results and to confirm the data already achieved in recent years, since one among th limitations found in the following systematic review conducted was the absence of control groups.
Corresponding author
Manila Caramazza, caramazzamanila1@gmail.com
Authors’ contributions
All authors contributed equally.
Declaration of conflict of interest
The authors declare no conflict of interest.