

Introduction
With the arrival of COVID-19, and its rapid spread worldwide.1 There were more than 18,142,000 confirmed cases of COVID-19 and more than 691,000 deaths, affecting 212 countries and territories. With a high rate of infection and deaths, COVID-19 can lead to many psychological problems including stress, anxiety, depression, fear, and possibly exhaustion.1 To prevent such psychological problems, it is important to understand the factors associated with individuals’ experience of stress and burnout during the COVID-19 pandemic. There is recent research that has shown that people who were in quarantine developed several psychological problems such as fear, stress, frustrations.2 On the other hand, the microbiome has co-evolved in the health of the host to be sustainable.3 The authors mention that the coronavirus disease 2019 (COVID-19) pandemic has generated 7,802 confirmed cases and 489 deaths in our Tumbes Region, and this has also caused stress in each person from of family, studies and work; This mental illness being of little importance for the Peruvian state.4
In Peru, in this quarantine of the COVID 19 pandemic, we have been exposed to many stressors every day, such as: mental and physical health, economic, family, work, states or problems, unforeseen events, variations in routine, experiences, activities. and inappropriate interpersonal relationships; which every living being faces in a different way, undoubtedly harming its function by not knowing how to proceed in the face of various stimuli and within the environment it inhabits, fatigue, exhaustion, high tension and excessive struggle are added.5
Research on the fecal microbiota of an individual with chronic stress influences memory in recipient hosts and this action may be related to the Alistipes genus.6
Taken together, these data strongly suggest a beneficial role of prebiotic treatment for stress-related behaviors. Furthermore, the gut microbiota supports therapeutic targeting for gut-brain axis disorders, opening new avenues in the field of nutritional neuropsychopharmacology.7 The gut microbiota composition of donor and recipient mice was also related to neuroinflammatory activity, resulting in a link between genetic modification, brain function, anxiety and depression.8 In recent years, research has been carried out on the human intestinal microbiota and its influence on Autism, Parkinson’s and Alzheimer’s. However, to date there is no research on the change in the composition of the intestinal microbiota that triggers stress, for its correct treatment.6 This is a very active area of research that holds promise for more effective, precision treatment of these stress related disorders in the future.9
The consequence of stress would be an irremediable state typical of human experience, becoming one of the important characteristics in the vision of mental and physical illnesses, generating a negative effect on the autonomic nervous system, which causes biochemical variations and hormonal changes that They damage the endocrine and immune system, and consequently the health of people.5,10
Materials and Methods
Population
States that the population is the set of all events that resemble a certain characteristic to be studied.11 In this sense, the population was made up of 197 adults between 18 and 59 years old.
Sample
Taking,11 as a reference, the sample is a subgroup of the world or population from which data is collected and which must be of a form peculiar to it. For the preparation process of this work, the sample was for convenience, selecting 40 adults. The study used case studies of 20 people with chronic stress and controls of 20 people who do not have chronic stress.
Data collection techniques and instruments Techniques
In the research, the survey technique was used,12 define: “It is a technique that depends on direct or indirect contact with all people whose attitudes, behaviors or characteristics are significant for a given investigation”.
Validity of the scale.
Validation by experts from 11 psychology professionals with clinical experience.
Technical methods and data collection instruments
In the collection of information, it was possible to capture each of the participants who belong to the sample, providing them with an explanation and the methodology that was carried out in the research, this with the objective that the participant has optimal knowledge of what will be carried out. and request permission so that it can be part of the application of the proposed instruments, which will be applied virtually.
Procedure Sampling
A total of 40 samples were collected; 20 of people with chronic stress and 20 people without chronic stress. The fecal samples were taken aseptically in the morning, each patient delivered a 2 g fecal sample by spontaneous evacuation into collection bottles that will contain 5 mL of RNA Later stabilization solution (Invitrogen™) and were frozen immediately until analysis.
Extraction of DNA
Fecal genomic DNA was extracted from the frozen samples according to the Geneaid cfDNA/cfRNA extraction kit following the manufacturer’s instructions (Presto™) and the amount of DNA was quantified using the UV spectrophotometer (Thermo ScientificTM NanoDropTM One).
Polymerase chain reaction (PCR)
The molecular identification of the bacteria was carried out by PCR amplification, using the extracted
DNA. The reactions were constituted in a final volume of 25 μL, which contained: 2.5 μL of Buffer10X (10 mM Tris-HCl, 50 mM KCl, 1.5 mM MgCl2, pH 8.3), 2.5 μL MgCl2 at 25 mM , 0.5 μL dNTPs at 10 mM, 16.2 μL AUP (Ultrapure Water), 0.6 μL Primer Forward 27F (AGA GTTTGA TCM TGG CTC AG) and 0.6 μL Primer Reverse 1492R (GGT TACCTT GTT ACGACTT) of the 16S rRNA Gene,13 0.1 μL Taq DNA polymerase (Invitrogen) and 2 μl of bacterial DNA. All of this was carried out in a Thermocycler (BIOMETRA UNO-Thermoblock) under a schedule of 35 cycles with a predenaturation temperature of 95°C for 5 min, 35 denaturation cycles at 95°C for 30 sec, Hybridization 58 °C for 45 sec), Polymerization 72°C for 1min 30 sec., plus a final Extension step of 72°C for 4 min. The PCR products were confirmed using the 1.5% agarose gel electrophoresis technique and the bands were visualized with Ethidium bromide staining in a UV Transilluminator.
Sequencing and bioinformatics procedure
These amplified PCR products were sent for analysis. Firstly, an Illumina DNA library was prepared and sequencing was performed in MR. DNA (www.mrdnalab.com, Shallowater, TX, USA), on a MiSeq following the manufacturer’s guidelines. Sequence data were processed using an MR DNA analysis pipeline. (ADN MR, Shallowater, TX, USA).
Once the sequences were obtained, they were analyzed using a bioinformatics program. First, for quality control, the Qiime2: DADA2 plugin was used to filter and correct any errors that these sequences may have. Input or raw sequences were first filtered by size based on a quality score greater than q35. Then the noise was eliminated from these, reducing the sequence errors, and likewise, the reads with the same sequences were grouped into unique sequences. Finally, chimeric sequences were eliminated, which resulted from the joining of more abundant sequences during sequencing.
Ethical considerations
It was good to follow the statutes referred to in the code of ethics of the psychologist of Peru, which subscribe that, in cases of research, the right to anonymity of the participants is respected as well as the decision not to conclude with the participation of the research if the participant so decided. For this reason, before completing the questionnaire, the participants were presented with an informed consent which explained that the identity of each of them was safeguarded (College of Psychologists of Peru, 2017).
Results
In table 1, we observe that of the total sample of 197 adults it is shown that 15.2% of the respondents do not present levels of stress, while 23.8% have mild psychosomatic distress, 39% have moderate psychosomatic distress and 22% chronic psychosomatic stress.
In table 2, age shows that 67.5% of those surveyed present chronic stress in young adults, 22.5% in adults and less incidence in older adults. In terms of sex, 75% are predominantly women and 25% are men, in residence 75% come from urban areas and 25% come from rural areas, level of education 30% are people with a degree of completed higher education ( professionals), 12.5% complete secondary school.
DNA metabarcoding analysys
Molecular identification and comparison of the bacterial microbiome, in individuals with stress (SC) and without stress (SE) at the sex level. Note: “Others” represent bacterial orders grouped less than 3%. The fecal bacterial microbiome identified at the molecular level in 20 individuals with stress (EC 01 to 20) and 20 individuals without stress (SE 01 to 20), according to sex, 30 female patients and 10 male patients.
In female patients with stress (SC) and without stress (SE), the bacterial orders Oscillopirales,
Bacteriodales and Lachnospirales at the intestinal level are the most predominant. However, Aeromonadales has a greater predominance in patient SE 14. The predominance of Lactobacillales bacteria in the patient with stress CE 05 and without stress SE 06. In male patients with stress (CE) and without stress (SE), in the bacterial orders Oscillopirales, Bacteriodales and Lachnospirales at the intestinal level are the most predominant. However, Aeromonadales is predominant in the patient with stress CE 12 and patient without stress SE15. Furthermore, Lactobacillales bacteria are predominant in patients with stress CE 11 and in those without stress SE 02. See figure 1.
At the level of rural residence in 10 patients from the rural area and 30 patients from the urban area, the bacterial microbiome identified in patients with stress (SC) and without stress (SE).

Note: “Others” represent the bacterial orders grouped less than 3%. In rural areas, the bacterial orders Oscillopirales, Bacteriodales and Lachnospirales at the intestinal level are the most predominant. However, Aeromonadales has a greater predominance in patient SE 14. The predominance of Lactobacillales bacteria in the patient with stress CE 04 and CE 05.
In the urban area, the bacterial orders Oscillopirales, Bacteriodales and Lachnospirales at the intestinal level are the most predominant. However, Aeromonadales has a greater predominance in patient CE 03. The predominance of Lactobacillales bacteria in the patient with stress CE 11 and SE See figure 1.
At the educational level in 05 complete secondary patients, 30 complete upper secondary patients and 05 incomplete upper secondary patients, the bacterial microbiome was identified in patients with stress (CE) and without stress (SE).
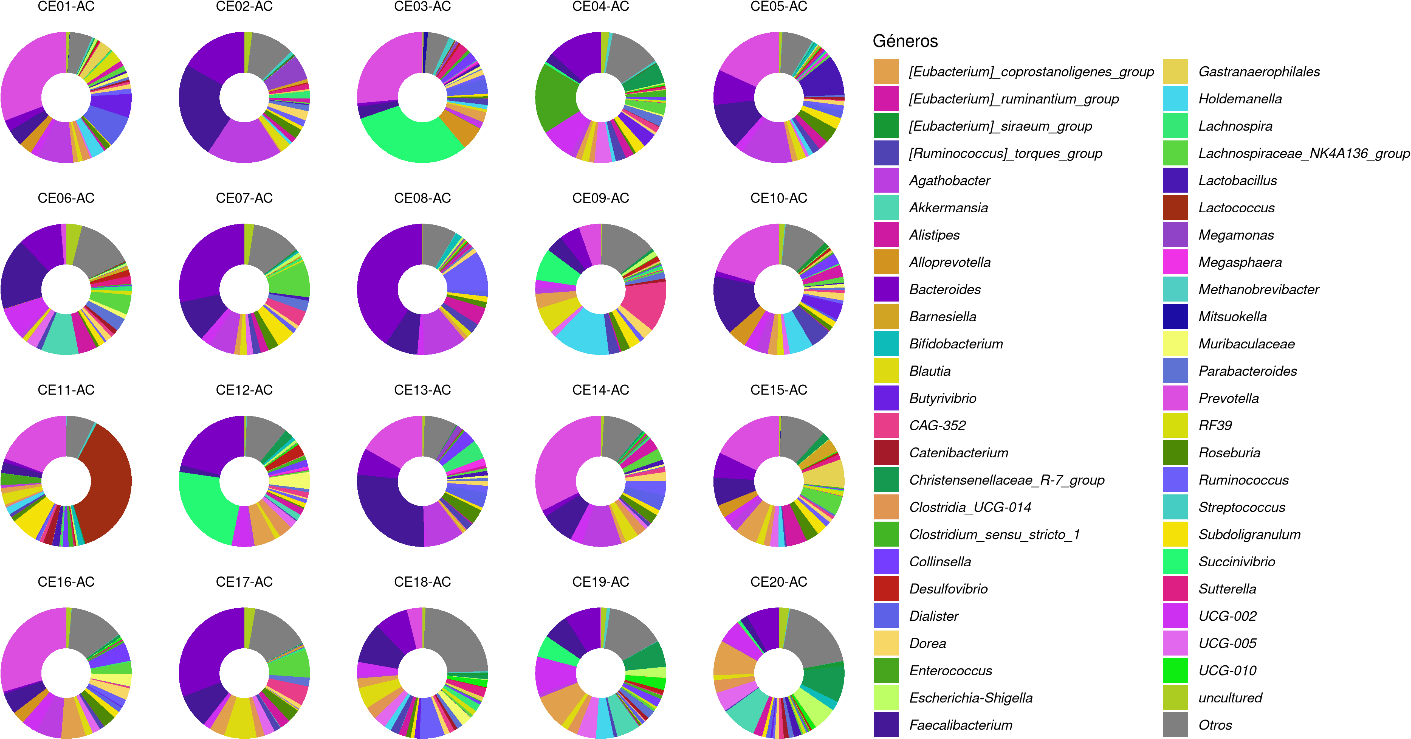
Molecular taxonomic classification of genera of individuals with and without stress. “Others” represent the genres grouped less than 3%
At the molecular level, the results in patients with stress (SC) and without stress (SE) in Figure 01 show 50 microbial genera with greater predominance (each color indicates a bacterial genus). The numbers 1 to 20 represent each patient. Others
Bacterial genera less than 3% were grouped into others, the identification of these bacterial genera is at the genomic level directed at the 16S rDNA gene.

In 20 patients without stress (SE), at the level of bacterial genus of the intestinal microbiome, the diversity of 49 bacterial genera is presented with greater predominance, 01 genus as uncultured (not cultured) means that this bacteria does not grow in a culture medium. Other bacterial genera less than 3% were grouped into others. See Figure 02.
In patients without stress (SE) and with stress (SC), different bacterial genera are present in the fecal microbiome; However, the bacterial genus Asteroleplasma is only present in patients without stress but not in patients with stress. See figure 02 and 03.
In patient SE 01, the most predominant bacterial genus is Escherichia-Shigella.
In patient SE 02, the most predominant bacterial genus is Prevotella.
In patient SE 05, the most predominant bacterial genus is Prevotella.
In patients SE 10, 13, 16,17, 18 and 19, the most predominant bacterial genus is Megamonas. In patients SE 14 and 15, the most predominant bacterial genus is Succinivibrio.

In 20 patients with stress (SC), at the level of bacterial genus of the fecal microbiome, the diversity of 48 bacterial genera is presented with greater predominance, 01 genus as uncultured (not cultured) means that this bacteria does not grow in a culture medium. Other bacterial genera less than 3% were grouped into others. See figure 03.
The bacterial genus Bifidobacterium and Alistipes are present in patients with stress
Figure 03 shows the diversity of bacteria present in patients with stress; However, some patients have more predominant bacterial genera as mentioned below.
In patients CE 01, 05, 10, 11, 13, 14, 15 and 16, the predominant bacteria is Megasphaera. In patient CE 02, the predominant bacteria is Faecalibacterium. In patients CE 03 and 12, the predominant bacteria is Lachnospira. In patients CE 07, 08 and 17, the predominant bacteria is Megamonas. In CE 11 patients, the predominant bacteria is Lactococcus.
Discussion
The difference in the DNA metabarcoding analysis of stress in healthy individuals and those with chronic stress from the fecal microbiome during the COVID-19 pandemic, Tumbes 2022. At the molecular level, they present the level of bacterial genera present in the fecal microbiome in patients with stress (CE ) we find the bacterial genus Asteroleplasma are found in individuals without stress. On the other hand, in patients with chronic stress we observed the bacteria Bifidobacterium and Alistipes are present in patients with chronic stress.
We found similar research focusing on the identification of the microbiome in stress patients according to,14 likewise15–17 in the advances of stress and depression during the last 18 months, the finding was reinforced by the deregulation of several biological systems, focusing on the link of stress with the gut microbiome. Similar research is found,18 their objective was to determine the maternal factors involved in maternal stress, anxiety and depression, their results revealed that babies of mothers who reported higher anxiety and perceived stress had reduced alpha diversity. Furthermore, the relative taxonomic quantitative abundances of Bifidobacterium dentium is associated with the modulation of the gut-brain axis, in both groups the genus Bifidobacterium was found.
Investigated the fecal microbial characteristics associated with mental health outcomes with symptoms of anxiety, depression or post-traumatic stress disorder in the Spanish population, these findings will help identify the microbial community being the bacterial genus Turicicbacter. The results reported for the Bifidobacterium Alistipes bacteria in patients diagnosed with chronic stress differ.19 Furthermore, it is mentioned that fecal indole-3-acetate is higher in patients with mental distress and correlates with intestinal dysfunction. These findings uncover a microbe-mediated gut-brain pathway that could be therapeutically targeted to stress-induced gut-brain comorbidities.20–22 Further investigations are needed in the field of the gut microbiome for the elucidation of the mechanisms by which gut dysbiosis contributes to the pathophysiology of neuropsychiatric disorders.23,24 In adiccion stress is related to socio-economic adversity - but not overall early life stress - is associated with a less diverse microbiome in the general population.25,26
The specific objective is to identify stress levels in individuals during the COVID-19 pandemic, Tumbes 2022. We found in a population of 197 individuals, 15.2% of individuals do not present stress, while 22% do not present chronic psychosomatic stress. Likewise, in the convenience sample there are individuals without stress and people with chronic stress. Similar studies were found according to anxiety, depression, stress and perception of health status were evaluated in Mexican university students, symptoms (moderate to severe), stress (31.92%) were found, especially in the group of women.27
In the objective: To compare molecularly and the bacterial microbiome in individuals without stress and with stress, according to sex, residence and level of education, 67.5% occurs in young adults (18 to 30 years old), with a greater predominance in the gender of women, being of greater relevance in urban areas followed by rural areas, educational level 30% with completed higher education (professional). Similar studies of the study of sociodemographic characteristics show that there is a prevalence of women up to the age of 30 who reside in an urban area, without children and with a complete higher education, carried out in the research,28 in which the results showed be relevant. In accordance with these results, it was found that in the study the majority of the population that presents distress are women who reside in the urban area.29 The results differ from those obtained where the predominant educational level was primary education.30
Conclusion
the bacteria Alistipes and Bifidobacterium are candidates as possible markers of the intestinal microbiome in patients with chronic stress, and the bacteria Asteroleplasma are candidates as a bacterial marker of the intestinal microbiome in healthy people. Finally, the identification of the microbiome in patients with stress opens a new path to understanding stress and its relationship to dysregulation with the microbiome.
Ethics Approval and Consent to Participate
Ethics approval for this study involving healthcare professionals was granted by the National University of Tumbes. The study was reviewed and approved adhering to the ethical standards of the responsible committee on human experimentation. Informed consent was obtained from all individual participants included in the study. Before participation, all healthcare professionals were provided with detailed information about the study’s aims, methodology, potential impacts, and their role in the research. Consent was documented in a manner that upholds the confidentiality and autonomy of all participants.
Consent for Publication
This study did involve patients, the anonymised results of the study to be published in academic journals and presented at conferences. The consent process assured participants that all data would be presented in such a way that individuals could not be identified, in accordance with privacy regulations and intitutional policies.
Competing interest
The authors declare that they have no financial or personal relationships that may have inappropriately influenced them in writing this paper.
Authors’ contributions
M.V. B and F.F conceived the study, carried out the analysis and wrote the first draft. F.Z and E.L.E administered the questionnaires and contributed to the final draft. A.E.P and M.M supervised the study, verified the analysis and contributed to the final draft.
Funding information
This research was funded by Resolution No. 0162-2021-UNTUMBES-R, in addition, this publication is part of EER undergraduate thesis at the Universidad National University of Tumbes.
Data availability
The anonymised data upon which this paper is based are available upon reasonable request from the corresponding author (F.F)
Disclaimer
The views and opinions expressed in this paper are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
Acknowledgments
This research was funded by Resolution No. 0162-2021-UNTUMBES-R, in addition, this publication is part of EER undergraduate thesis at the Universidad National University of Tumbes.
Correspondence should be addressed to:
Fredy Fabian Domínguez, cell phone: +51 962644603 ffabian@unsm.edu.pe