Introduction
In fostering healthier communities, understanding the factors that drive individuals to commit to positive health trajectories is paramount.1–7 A clinician’s job is to care for their patients, motivate them to take charge of their health, and educate them on how to keep their bodies healthy.1,4,6 However, how does one explain the same idea to hundreds of people from every walk of life? Each patient is unique. By understanding key motivators for large demographics, physicians can enhance patient-physician relationships and provide better, higher-quality care to the patient.2,7
Motivational factors that drive patient behaviors are multifaceted. Core elements include intrinsic motivators, such as a patient’s personal desire for wellness and quality of life, and extrinsic motivators, like social support and healthcare incentives. Physicians should encourage the development of self-efficacy, helping patients believe in their ability to make changes. Empathy and understanding from clinicians can bolster a patient’s motivation, as can culturally sensitive communication that respects individual beliefs and preferences. Setting achievable goals and providing clear, actionable advice can create a sense of empowerment. Additionally, leveraging technology for reminders and tracking progress can sustain motivation over time. By acknowledging and supporting these motivational factors, physicians can foster sustained engagement in health-promoting behaviors among their patients. The first step is to examine the personal motivators for patients to maintain their health, which is the aim of this national survey study.
Methods
Recruitment data collection
This survey polled 204 residents of the United States over the age of 16. The participants answered questions about their chronic health conditions, current state of health, frequency of doctor visits, and motivations for health. The participants were asked to rank a subject’s significance on a scale of one to five to gauge receptiveness to the idea or subject.
Statistical analyses
Statistical analyses were performed using JMP Pro 17 for Mac OS.
The Survey
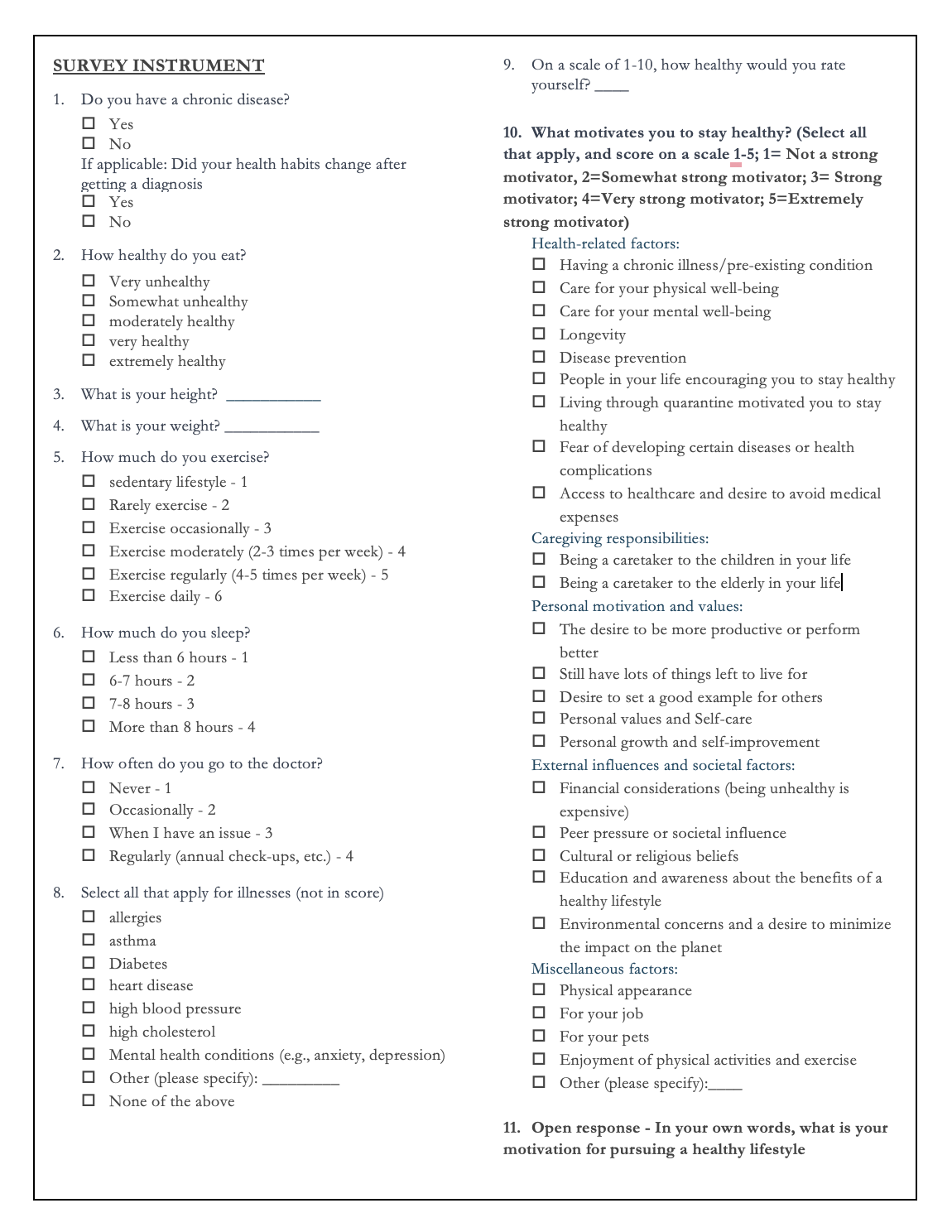
The survey consisted of 15 questions [Figure 1]. The first and second questions asked if the participant had a chronic illness and if their lifestyle changed after diagnosis. Both of these were “yes” or “no” questions. The third and fourth questions asked the participants to input their height and weight, which was used to calculate their basal metabolic index (BMI). Questions five through nine were questions regarding the health habits of the participants. They were asked to select the statement that best applies to them concerning the question being asked. These questions asked about sleep, dietary, and exercise habits and how often they go to the doctor. The data collected from these questions helped sort participants into categories based on their answers. We then asked how healthy the participants would rate themselves on a scale of one through ten for the same reason. Questions ten through fourteen asked the participants to rate how the following statements apply to them on a scale of one to ten: Health-related factors, caregiving responsibilities, personal motivation and values, external influences and societal factors, and miscellaneous factors. The final question was, “in your own words, what is your motivation for pursuing a healthy lifestyle.”

Results
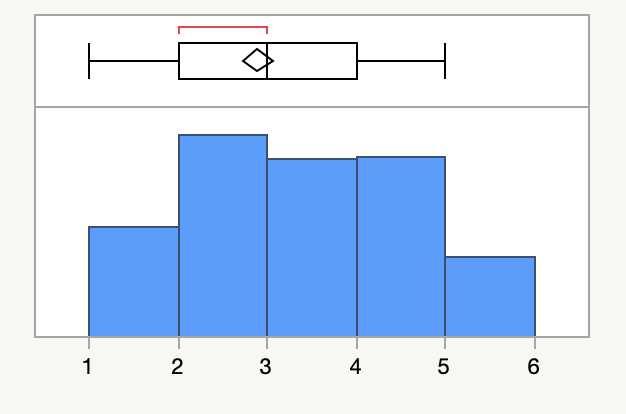
The median age of the cohort was 41 years, with an interquartile range of 23 - 25. There was a much larger female population than male, with 68% of the participants being female and 30% male. The ethnoracial composition was 64.5% White, 15% Black, 9.5% Asian, 4.5% Latino, 1.5% Arab, and 5% selected “other.” “Prefer not to say” and mixed race were tied, only being selected by 0.5% of the cohort. This composition is similar to the 2022 United States Census Bureau statistics, except that “White” would be expected to be closer to 75%; this could be because of the choices of Latino, Arab, and Other being available. We expected a majority of the cohort to have one child since that is the average number of children in an American household. However, 77.5% of the cohorts had no children, 12% had one kid, 19% had two kids, 9% had three kids, 4.5% had four kids, and 2% had six or more kids. This likely reflects a declining US birth rate with fewer families opting for children.
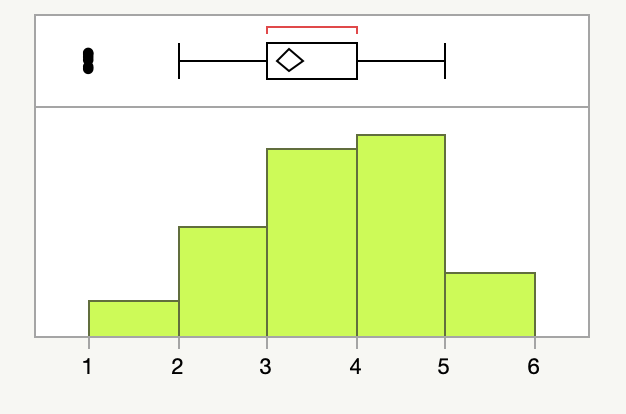
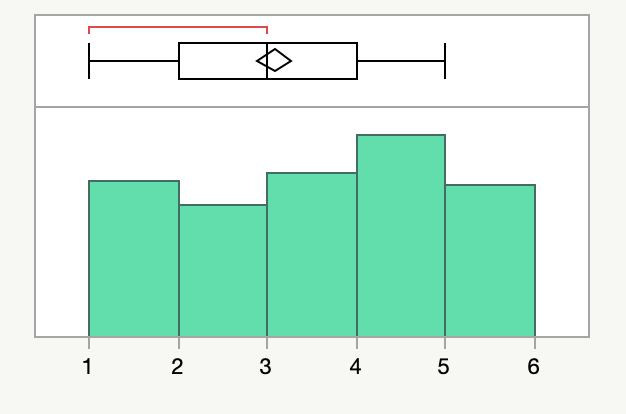
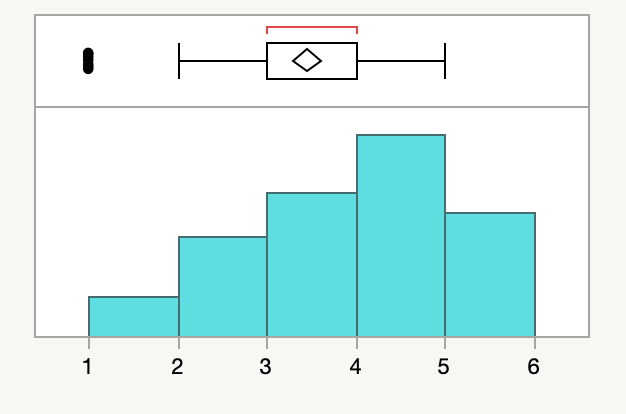
Various factors motivate individuals to be healthy [Figure 2].




In general, personal motivation was the most motivating factor for the cohorts. Examples of “personal motivations and values” in this category included career goals, weight loss, and cosmetic goals. The focus on career-related health maintenance made sense, given that 60% of participants held blue-collar jobs, necessitating maintaining their health. In the words of one participant, “I wish to stay healthy so that I can continue to work, protect, and take care of my family.”
Caregiving responsibilities were the second most powerful motivator. On a scale of one to five, the mean response for this category was 3.85, and 41% of respondents gave it a five for importance. The gender distribution was very intriguing when analyzing this section. On a scale of one to five, 36.54% of women gave caregiving for children or the elderly a five for importance. On the other hand, only 20% of men gave it a five out of five for importance. “personal motivation and values,” described as “the desire to be more productive or perform better; desire to set a good example for others; Personal growth and self-improvement,” received the most fives from men.
Health-related motivation was ranked third overall. Our survey defined health-related factors as the desire to maintain good health due to a chronic illness or a propensity for specific chronic conditions. On a scale of one to five, this received a five from 44% of participants, with a mean rating of 3.38. The survey question on chronic illness provided evidence for these figures. 31.38% of participants had a chronic illness, and 68.09% of those 31.4% made changes to their lifestyle post-diagnosis. In light of this, many of the short answer responses from people with chronic illness listed it as a personal motivator. To quote a female participant," I have diabetes. I want to be healthy and live a long life." Another participant who had a predisposition to high blood pressure and obesity said that he maintains his health as a preventative procedure against illness."
“External Influences and Societal Factors” appeared to be the least inspirational category. Examples for this category included concerns about one’s physical appearance, money, peer pressure or societal influence, cultural or religious beliefs, education about the advantages of leading a healthy lifestyle, environmental issues, or a desire to have as little impact as possible on the environment. Only 40% of participants gave this a perfect score; the average was 3.67. Only 34.6% of responses in the short answer reflected these values, which indicated this. One participant stated, “I want to feel like my ideal self and carry myself confidently, which is why I am pursuing a healthy lifestyle. If I look good, I will always feel good.” By emphasizing the importance of their appearance, they emphasized their desire for a healthy lifestyle. Another participant said about an outside factor like religion, “my faith is my greatest motivation.” When acknowledging these values, it is critical to remember that most people had chronic conditions or a propensity for chronic illness, so it makes sense that it would be less of a concern for the general cohorts.
Discussion
The study investigated the motivating factors driving individuals to pursue a healthy lifestyle. The analysis revealed several key factors that influenced participants’ choices, with “personal motivation and values,” “caregiving responsibilities,” and “health-related concerns” emerging as the primary drivers.
Understanding the motivation behind health behavior change is a critical aspect of public health and clinical practice. With the rise of lifestyle-related chronic diseases, researchers and clinicians are increasingly interested in the psychological and neurobiological underpinnings of such motivation. According to an integrative review by Esch and colleagues, motivation and reward systems play a crucial role in behavior change, including the pursuit of health-related goals. They describe three core motivational systems: the desire for pleasure, the desire for relief from aversion, and the desire for assertive quiescence when a new behavior becomes habitual. These systems are involved in different stages of the behavior change process and are influenced by emotions, affect, and learning, suggesting that both appetitive and aversive motivational salience can be activated during the engagement phase of behavior change.8
Recent advances in neuroscience have shed light on the neurobiological mechanisms that underpin motivation and reward processes related to health behavior change. This body of work integrates neurobiological science with social psychological literature on behavior change, presenting models that consider motivation and reward mechanisms. Such an approach underscores the importance of factors like delayed gratification, self-regulation skills, self-efficacy, and internal locus of control in pursuing health behavior changes.9
Damrosch’s research from the field of health psychology has provided insights into strategies for motivating health behavior change. Factors such as the perceived severity of a health threat, personal vulnerability, and the perceived effectiveness of health measures have been confirmed to be significant in motivating individuals to change behaviors. Self-efficacy, which is the belief in one’s ability to succeed, is also a key predictor of outcomes such as smoking cessation and increased physical activity after a heart attack. However, the role of fear in motivating behavior change remains complex, with high levels of induced fear potentially leading to denial or inaction unless coupled with effective behavior change strategies.10
These findings collectively highlight that motivation for health behavior change is a complex interplay of cognitive, emotional, and neurobiological factors. Interventions aimed at improving health behaviors must, therefore, address these multifaceted aspects of motivation, emphasizing not only the acquisition of knowledge and skills but also tapping into the intrinsic and extrinsic rewards that drive behavior change. Our study provides personal context to the factors that motivate individuals to be healthy, a starting point for any of these health interventions.
Conclusion
Understanding the diverse motivating factors that drive individuals to pursue a healthy lifestyle can significantly enhance patient-physician relationships. This insight allows healthcare providers to establish a more empathetic and patient-centered approach tailored to individual motivations and values. By recognizing the primary motivating factors for each patient, physicians can craft personalized care plans that resonate with their patients’ aspirations and concerns. Incorporating a patient’s motivations into the treatment plan fosters a more open and trusting patient-physician relationship and enhances treatment adherence and outcomes by aligning healthcare recommendations with patients’ intrinsic drivers.